

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Erdheim-Chester disease (ECD) is a rare disease that is characterized by multi-organ involvement of foamy histiocytes. It causes systemic inflammation, and also demonstrates various clinical manifestations and has a poor prognosis. We encountered a case of ECD in a patient that had been treated for underlying polycythemia vera. As far as we know, this is the first reported case worldwide where ECD developed in association with polycythemia vera. A 59-year-old man visited our hospital due to pleuric pain at the right side of the chest. Pleural tissue that was obtained following a thoracoscopic biopsy showed non-Langerhan's cell histiocytosis, suggesting the presence of ECD. The histiocytes stained positively for CD68, but were negative for S-100 and CD1a. The patient also complained of pain at both hips and the right shoulder area. An X-ray and magnetic resonance image demonstrated that the lesion showed sclerosis and osteolysis in both the proximal femur and right humerus. Treatment was started with predinisolone, and subsequently cyclophosphamide was added. ECD is a very rare multi-systemic disease, and its cause and therapeutic options have not yet been defined. ECD has a poor prognosis. Therefore, we believe that additional case studies are needed prior to the determination of a novel therapy for ECD.
Figures and Tables

Figure 2
Chest CT shows large amount of right pleural effusion and surrounding pleural thickenings. Small amount of pericardial effusion are also noted (A). Focal wall thickening and enhancement is seen at lateral wall of aorta and bilateral perirenal fat infiltrations combined with bilateral pelvic dilatations are noted which represent bilateral nephritis and mild hydronephritis (B).

Figure 3
(A) Pelvis X-ray shows ill-defined sclerosis and osteolysis in both pubic bone and proximal femur metadiaphysis. (B) Right humerus AP X-ray also shows diffuse sclerosis in proximal humeral shaft.

Figure 4
Coronal (A) and axial (B) T-1 wieghted pelvic bone MRI shows numerous variable sized (less than 1 cm to 7 cm) round oval to ill-defined patchy marrow signal changes (arrow) involving the L4-5 body and other multiple lesions in pelvic bone. Lesions appear relatively dark signal intensity on T1-wighted image.

Figure 5
Bone scan shows multifocal hot uptake in right humeral neck, right side of L5-S1 vertebrae, right 7th-9th costovertebral junction areas, left iliac bone, and left 5th posterior rib. A focal hot uptake in right humeral head, and right 7th axillary rib is again seen. Periarticular areas of bilateral hips show increased activity.

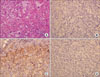
Figure 6
Pleural biopsy, (A) there are diffuse lipid-laden histiocyte infiltration, and Touton- type multinucleated eosinophilic giant cell (arrow) (H&E stain, ×200). (B) Immunohistochemical staining of S-100 protein reveals cytoplasmic staining only few macrophages (S-100, ×200). (C) Immunohistochemical staining of CD68 demonstarates strong positive, expressed as brown color in most macrophages (CD-68, ×200). (D) Immunohistochemical staining of CD1a reveals negative result (CD1a, ×200).
References
1. Devouassoux G, Lantuejoul S, Chatelain P, Brambilla E, Brambilla C. Erdheim-Chester disease: a primary macrophage cell disorder. Am J Respir Crit Care Med. 1998. 157:650–653.
2. Allen TC, Chevez-Barrios P, Shetlar DJ, Cagle PT. Pulmonary and ophthalmic involvement with Erdheim-Chester disease: a case report and review of the literature. Arch Pathol Lab Med. 2004. 128:1428–1431.
3. Hwang HS, Ji BS, Lee CK, Kim JY, Choi BS, Yang CW, et al. A case of Erdheim-Chester disease that presented with chronic renal failure. Korean J Med. 2007. 73:216–222.
4. Kim YJ, Kim YD. Erdheim-Chester disease: two cases of orbital involvement. J Korean Ophthalmol Soc. 2002. 43:1323–1329.
5. Park YK, Ryu KN, Huh B, Kim JD. Erdheim-Chester disease. J Korean Med Sci. 1999. 14:323–326.
6. Hong JR, Lee HG, Ko YH, Ahn JM, Choi YH, Kim BT. A case of Erdheim-Chester disease with periodic fever and knee pain. Korean J Med. 1999. 56:542–546.
7. Veyssier-Belot C, Cacoub P, Caparros-Lefebvre D, Wechsler J, Brun B, Remy M, et al. Erdheim-Chester disease. Clinical and radiologic characteristics of 59 cases. Medicine (Baltimore). 1996. 75:157–169.
8. Sheu SY, Wenzel RR, Kersting C, Merten R, Otterbach F, Schmid KW. Erdheim-Chester disease: case report with multisystemic manifestations including testis, thyroid, and lymph nodes, and a review of literature. J Clin Pathol. 2004. 57:1225–1228.
9. Favara BE, Jaffe R. Pathology of Langerhans cell histiocytosis. Hematol Oncol Clin North Am. 1987. 1:75–95.
10. Chung JH, Park MS, Shin DH, Choe KO, Kim SK, Chang J, et al. Pulmonary involvement in Erdheim-Chester disease. Respirology. 2005. 10:389–392.
11. Athanasou NA, Barbatis C. Erdheim-chester disease with epiphyseal and systemic disease. J Clin Pathol. 1993. 46:481–482.
12. Koziolek MJ, Kunze E, Muller A, Thiem V, Scheel AK, Muller D, et al. Erdheim-Chester disease. Dtsch Med Wochenschr. 2005. 130:25–28.
13. Bourke SC, Nicholson AG, Gibson GJ. Erdheim-Chester disease: pulmonary infiltration responding to cyclophosphamide and prednisolone. Thorax. 2003. 58:1004–1005.
14. Boissel N, Wechsler B, Leblond V. Treatment of refractory Erdheim-Chester disease with double autologous hematopoietic stem-cell transplantation. Ann Intern Med. 2001. 135:844–845.
15. Braiteh F, Boxrud C, Esmaeli B, Kurzrock R. Successful treatment of Erdheim-Chester disease, a non-Langerhans-cell histiocytosis, with interferon-alpha. Blood. 2005. 106:2992–2994.
 XML Download
XML Download