

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
A sarcoidosis is a multisystemic granulomatous disorder that has a predilection for pulmonary involvement, and the common radiological findings for the disease are bilateral nodular or reticulonodular patterns. Pseudoalveolar sarcoidosis is a rare presentation of sarcoidosis. The radiological finding is an alveolar pattern that involves or compresses the alveoli by clustered interstitial granuloma. A 58-year-old man was admitted due to incidental findings of a unilateral consolidative lesion as seen on chest radiography. A chest computed tomography (CT) examination showed multiple bronchoalveolar consolidations that were suspicious of a malignancy. However, a percutaneous needle biopsy revealed non-caseating granuloma with an asteroid body that was compatible with sarcoidosis. After one month, the consolidative lesions improved without any treatment.
Figures and Tables
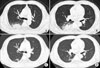
Figure 1
(A) Initial chest X-ray shows a consolidation of the right lower lung field. (B) A follow-up chest X-ray (1 month later) shows a partial resolution of consolidation of the right lower lung field.


References
1. Johkoh T, Ikezoe J, Takeuchi N, Kohno N, Tomiyama N, Akira M, et al. CT findings in "pseudoalveolar" sarcoidosis. J Comput Assist Tomogr. 1992. 16:904–907.
2. Muller NL, Mawson JB, Mathieson JR, Abboud R, Ostrow DN, Champion P. Sarcoidosis: correlation of extent of disease at CT with clinical, functional, and radiographic findings. Radiology. 1989. 171:613–618.
3. Sahn SA, Schwarz MI, Lakshminarayan S. Sarcoidosis: the significance of an acinar pattern on chest roentgenogram. Chest. 1974. 65:684–687.
4. Grenier P, Valeyre D, Cluzel P, Brauner MW, Lenoir S, Chastang C. Chronic diffuse interstitial lung disease: diagnostic value of chest radiography and high-resolution CT. Radiology. 1991. 179:123–132.
5. Battesti JP, Saumon G, Valeyre D, Amouroux J, Pechnick B, Sandron D, et al. Pulmonary sarcoidosis with an alveolar radiographic pattern. Thorax. 1982. 37:448–452.
6. Nam JE, Ryu YH, Park JG, Choe KO, Im JG, Lee KS, et al. High resolution CT findings of pseudoalveolar sarcoidosis. J Korean Radiol Soc. 2002. 47:191–196.
7. Hamper UM, Fishman EK, Khouri NF, Johns CJ, Wang KP, Siegelman SS. Typical and atypical CT manifestation of pulmonary sarcoidosis. J Comput Assist Tomogr. 1986. 10:928–936.
8. Sharma OP. Sarcoidosis: a worldwide phenomenon. Sarcoidosis. 1984. 1:11–15.
9. Brauner MW, Grenier P, Mompoint D, Lenoir S, de Cremoux H. Pulmonary sarcoidosis: evaluation with high resolution CT. Radiology. 1989. 172:467–471.
10. Gibson GJ, Prescott RJ, Muers MF, Middleton WG, Mitchell DN, Connolly CK, et al. British Thoracic Society Sarcoidosis study: effects of long term corticosteroid treatment. Thorax. 1996. 51:238–247.
11. Newman LS, Rose CS, Maier LA. Sarcoidosis. N Engl J Med. 1997. 336:1224–1234.
 XML Download
XML Download