

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Pneumatosis intestinalis or spontaneous pneumomediastinum are rarely associated with nonspecific interstitial pneumonia (NSIP). However, the development of both conditions in the same patient simultaneously has not been reported previously. A 56-year-old man with NSIP developed spontaneous pneumomediastinum accompanied by subcutaneous emphysema and pneumatosis intestinalis after the treatment with intravenous high dose steroid. The development of spontaneous pneumomediastinum, subcutaneous emphysema and pneumatosis intestinalis in this patient was possibly due to the factors such as NSIP, high dose steroid therapy and subclinical dermatomyositis. Treatment with corticosteroid and cyclosporin gradually improved his exacerbated NSIP and pneumomediastinum, subcutaneous emphysema, pneumatosis intestinalis.
Figures and Tables
Figure 1
(A) Chest X-ray shows pneumonic consolidation on right lower lobe and suspicious faint nodular opacities on both lungs. (B) Chest CT shows irregular patchy airspace consolidation on peripheral portion of both lower lobes.
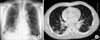
Figure 2
Pathologic finding shows mixed cellular and fibrotic NSIP. The uniform distribution is characteristic of both cellular and fibrotic NSIP (H&E stain, ×100).
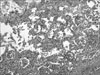
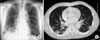
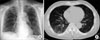
Figure 3
(A) Chest X-ray shows diffusely increased ground glass opacity on both lungs. (B) HRCT shows the aggravation of irregular patchy airspace consolidation, multiple ground glass opacities and reticular opacities on the peripheral portion.

References
1. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS Executive Committee, June 2001. Am J Respir Crit Care Med. 2002. 165:277–304.
2. Douglas WW, Tazelaar HD, Hartman TE, Hartman RP, Decker PA, Schroeder DR, et al. Polymyositis-dermatomyositis-associated interstitial lung disease. Am J Respir Crit Care Med. 2001. 164:1182–1185.
3. Kuroda T, Morikawa H, Satou T, Tanabe Y, Murakami S, Ito S, et al. A case of dermatomyositis complicated with pneumomediastinum successfully treated with cyclosporin A. Clin Rheumatol. 2003. 22:45–48.
4. Wada Y, Murayama N, Hirose S, In H, Kuroda T, Ito S, et al. A case of pneumatosis cystoides intestinalis in a patient with polymyositis and interstitial pneumonia. Mod Rheumatol. 2004. 14:260–263.
5. Won Huh J, Soon Kim D, Keun Lee C, Yoo B, Bum Seo J, Kitaichi M, et al. Two distinct clinical types of interstitial lung disease associated with polymyositis-dermatomyositis. Respir Med. 2007. 101:1761–1769.
6. Fujisawa T, Suda T, Nakamura Y, Enomoto N, Ide K, Toyoshima M, et al. Differences in clinical features and prognosis of interstitial lung diseases between polymyositis and dermatomyositis. J Rheumatol. 2005. 32:58–64.
7. Cottin V, Thivolet-Bejui F, Reynaud-Gaubert M, Cadranel J, Delaval P, Ternamian PJ, et al. Interstitial lung disease in amyopathic dermatomyositis, dermatomyositis and polymyositis. Eur Respir J. 2003. 22:245–250.
8. Neves Fde S, Shinjo SK, Carvalho JF, Levy-Neto M, Borges CT. Spontaneous pneumomediastinum and dermatomyositis may be a not so rare association: report of a case and review of the literature. Clin Rheumatol. 2007. 26:105–107.
9. Panacek EA, Singer AJ, Sherman BW, Prescott A, Rutherford WF. Spontaneous pneumomediastinum: clinical and natural history. Ann Emerg Med. 1992. 21:1222–1227.
10. Yamanishi Y, Maeda H, Konishi F, Hiyama K, Yamana S, Ishioka S, et al. Dermatomyositis associated with rapidly progressive fatal interstitial pneumonitis and pneumomediastinum. Scand J Rheumatol. 1999. 28:58–61.
11. Kono H, Inokuma S, Nakayama H, Suzuki M. Pneumomediastinum in dermatomyositis: association with cutaneous vasculopathy. Ann Rheum Dis. 2000. 59:372–376.
12. Hisamoto A, Mizushima T, Sato K, Haruta Y, Tanimoto Y, Tanimoto M, et al. Pneumatosis cystoides intestinalis after alpha-glucosidase inhibitor treatment in a patient with interstitial pneumonitis. Intern Med. 2006. 45:73–76.
13. St Peter SD, Abbas MA, Kelly KA. The spectrum of pneumatosis intestinalis. Arch Surg. 2003. 138:68–75.
14. Selva-O'Callaghan A, Martinez-Costa X, Solans-Laque R, Mauri M, Capdevila JA, Vilardell-Tarres M. Refractory adult dermatomyositis with pneumatosis cystoides intestinalis treated with infliximab. Rheumatology (Oxford). 2004. 43:1196–1197.
15. Miyake S, Ohtani Y, Sawada M, Inase N, Miyazaki Y, Takano S, et al. Usefulness of cyclosporine A on rapidly progressive interstitial pneumonia in dermatomyositis. Sarcoidosis Vasc Diffuse Lung Dis. 2002. 19:128–133.
 XML Download
XML Download