

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Tuberculous spondylitis is the most common manifestation of musculoskeletal tuberculosis (TB). The progression of the disease is usually slow and insidious. The main symptom, back pain, is not specific, which frequently results in a delayed diagnosis resulting in neurologic deficits and more advanced vertebral destruction. It is more difficult to diagnose the disease if the involved area is an uncommon sites, such as the upper thoracic, cervical or sacral region. It is important to make an early diagnosis and treatment to achieve a better treatment outcome. We reported a 29 year old female with upper thoracic TB spondylitis(T2-8) and pulmonary TB complaining of back pain that persisted for 5 months and fever. TB spondylitis was not suspected to be due to upper thoracic involvement despite her pulmonary tuberculosis. Chest CT for the evaluation of pulmonary TB found T5 destruction and the paravertebral abscess that was consistent with TB spondylitis. Her spine was examined by MRI, which made an early diagnosis before the neurologic deficit had developed. She was treated with surgical intervention due to the spinal instability and anti-TB medication for 1 year with excellent results.
Figures and Tables
Figure 1
Plain chest radiograph taken on admission shows increased infiltrative density on left lung.
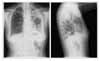
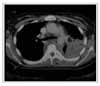
Figure 3
Spine MRI (left: T2 weighted image, right: T1 weighted image) shows compression fracture, fusion and kyphotic deformity of T5 and T6 and paravertebral abscess.


References
1. Weaver P, Lifeso R. The radiological diagnosis of tuberculosis of the adult spine. Skeletal Radiol. 1984. 12:178–186.
2. Janssens JP, de Haller R. Spinal tuberculosis in a developed country. A review of 26 cases with special emphasis on abscesses and neurologic complications. Clin Orthop Relat Res. 1990. 257:67–75.
3. Fancourt GJ, Ebden P, Garner P, Cookson JB, Wales JM, Stoyle TF. Bone tuberculosis: results and experience in Leicestershire. Br J Dis Chest. 1986. 80:265–272.
4. Omari B, Robertson JM, Nelson RJ, Chiu LC. Pott's disease. A resurgent challenge to the thoracic surgeon. Chest. 1989. 95:145–150.
5. Friedman B. Chemotherapy of tuberculosis of the spine. J Bone Joint Surg Am. 1996. 48:451–474.
6. Hoffman EB, Crosier JH, Cremin BJ. Imaging in children with spinal tuberculosis. A comparison of radiography, computed tomography and magnetic resonance imaging. J Bone Joint Surg Br. 1993. 75:233–239.
7. Pertuiset E, Beaudreuil J, Liote F, Horusitzky A, Kemiche F, Richette P, et al. Spinal tuberculosis in adults. A study of 103 cases in a developed country, 1980-1994. Medicine (Baltimore). 1999. 78:309–320.
8. De Vuyst D, Vanhoenacker F, Gielen J, Bernaerts A, De Schepper AM. Imaging features of musculoskeletal tuberculosis. Eur Radiol. 2003. 13:1809–1819.
9. Clementsen P, Hansen M, Conrad C, Myhre O. Percutaneous drainage of tuberculous abscess of the psoas muscle. Tubercle. 1988. 69:63–65.
10. Desai SS. Early diagnosis of spinal tuberculosis by MRI. J Bone Joint Surg Br. 1994. 76:863–869.
11. Sharif HS, Morgan JL, al Shahed MS, al Thagafi MY. Role of CT and MR imaging in the management of tuberculous spondylitis. Radiol Clin North Am. 1995. 33:787–804.
12. Hoffman KL, Bergman AG, Hoffman DK, Harris DP. Tuberculous tensosynovitis of the flexor tendons of the wrist: MR imaging with pathologic correlation. Skeletal Radiol. 1996. 25:186–188.
13. Medical Research Council Working Party on Tuberculosis of the Spine. A controlled trial of six-month and nine-month regimens of chemotherapy in patients undergoing radical surgery for tuberculosis of the spine in Hong Kong. Tubercle. 1986. 67:243–259.
14. Tuli SM. Results of treatment of spinal tuberculosis by "middle-path" regime. J Bone Joint Surg Br. 1975. 57:13–23.
15. Blumberg HM, Burman WJ, Chaisson RE, Daley CL, Etkind SC, Friedman LN, et al. Ameriacn Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med. 2003. 167:603–662.
 XML Download
XML Download