

 ePub
ePub Citation
Citation Print
Print


Abstract
Lung cancer, breast cancer and lymphoma are the common oncologic causes of malignant pleural effusion, comprising more than the half of the causes. However, an endocrinologic carcinoma associated malignant effusion is very rare. Recently, we encountered a case of papillary thyroid carcinoma causing malignant effusion. An 83-year-old female patient presented with dyspnea due to massive pleural effusion in her left side. The pleural biopsy, pleural fluid cytology and breast needle aspiration biopsy results were consistent with a metastatic papillary thyroid carcinoma. Thyroid ultrasonography showed two thyroid masses, but the patient refused a thyroid biopsy. This case highlights the need for considering the possibility of papillary thyroid carcinoma when the cause of malignant pleural effusion cannot be found because one of the rare clinical manifestations of a papillary thyroid carcinoma can be dyspnea due to malignant effusion.
Figures and Tables
Figure 1
Chest X-ray shows left pleural effusion and left upper mediastinal mass with tracheal deviation.

Figure 2
Chest CT shows a highly enhancing left thyroid mass with central low density (A), enlarged left axillary lymph node (large arrow) and pleural effusion with enhanced pleural nodule (small arrow) (B), and large left anterior chest wall mass with lung invasion (large arrow) and pleural nodules (small arrows) (C).
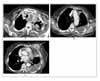
Figure 3
Thyroid ultrasonography shows isoechoic mass measuring 1 cm in the right thyroid (A), and large well-defined isoechoic mixed mass measuring 4.5 cm in the left thyroid (B).

Figure 4
On Hematoxylin and Eosin (H&E) stained tissue section of the pleural biopsy specimen, a few papillary clusters of atypical cells with abundant eosinophilic cytoplasm, prominent nucleoli, and occasional nuclear grooves are observed (H&E stain, × 400).



References
1. Vernon AN, Sheeler LR, Biscotti CV, Stoller JK. Pleural effusion resulting from metastatic papillary carcinoma of the thyroid. Chest. 1992. 101:1448–1450.
2. Hausheer FH, Yarbro JW. Diagnosis and treatment of malignant pleural effusion. Cancer Metastasis Rev. 1987. 6:23–40.
3. Kim JY, Park DW, Na JO, Hwang BY, Kim DL, Shin DH, et al. A Case of Malignant Pleural Effusion with Pleural Metastasis in a Patient with Papillary Thyroid Carcinoma. J Korean Soc Endocrinol. 2002. 17:269–274.
4. Lee KY, Myong NH, Kim KY. Occult Papillary Thyroid Carcinoma Presenting as a Metastatic Pleural Effusion. Tuberc Respir Dis. 1995. 42:594–599.
5. Nemec J, Zamrazil V, Pohunkova D, Zeman V, Rohling S. Mode of spread of thyroid cancer. Oncology. 1979. 36:232–235.
6. Massin JP, Savoie JC, Garnier H, Guiraudon G, Leger FA, Bacourt F. Pulmonary metastases in differentiated thyroid carcinoma. Study of 58 cases with implications for the primary tumor treatment. Cancer. 1984. 53:982–992.
7. Hyman MP. Papillary and undifferentiated thyroid carcinoma presenting as a metastatic papillary serous effusion. A case report. Acta Cytologica. 1979. 23:483–486.
8. Hoie J, Stenwig AE, Kullmann G, Lindegaard M. Distant metastases in papillary thyroid cancer. A review of 91 patients. Cancer. 1988. 61:1–6.
9. Vassilopoulou-Sellin R, Sneige N. Pleural effusion in patients with differentiated papillary thyroid cancer. South Med J. 1994. 87:1111–1116.
 XML Download
XML Download