

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Acute fibrinous and organizing pneumonia (AFOP) is a histological pattern consisting of prominent intra-alveolar fibrin and organizing pneumonia, with out hyaline membranes or prominent eosinophilia. The clinical manifestations of AFOP resemble those of acute lung injury such as acute interstitial pneumonia (AIP). However, the classic histological patterns of AFOP differ from diffuse alveolar damage (DAD), bronchiolitis obliterans with organizing pneumonia (BOOP) or acute eosinophilic pneumonia (AEP). The characteristic intra-alveolar fibrin ball and lack of classic hyaline membrane are the predominant histological features of AFOP. Although some reports suggest that its clinical course is less catastrophic than DAD, the clinical entity that distinguishes AFOP from DAD has not been established. We present a case of pathologically demonstrated AFOP in a 79-year-old man. The radiological findings of our case were similar to those of DAD, presented with diffuse bilateral lung infiltrations. However, despite the rapid development of respiratory failure, the patient had a better response and outcome to steroid therapy than what would be expected for DAD.
Figures and Tables
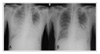 | Figure 1Chest PA. (A) Prominent bilateral asymmetric patchy infiltrations through both middle and lower lung fields were seen on admission. (B) After high-dose methylprednisolone therapy for 7 days, the parenchymal infiltrates through both lung fields are improved (extubation state).
|
 | Figure 2Computed tomography of chest. Diffuse, extensive ground glass appearance and fine reticular patterns were noted on both upper and lower lung fields.
|
 | Figure 3(A) Thoracoscopic lung biopsy of right middle and lower lobes. Exuberant intra-alveolar fibrin and organizing loose connective tissue involved more than 50% of air spaces with patchy distribution (H&E, ×40). (B) Thoracoscopic lung biopsy of right middle and lower lobes. Exuberant intra-alveolar fibrin and organizing loose connective tissue involved more than 50% of air spaces with patchy distribution (H&E, ×40).
|
References
1. Beasly MB, Franks TJ, Galvin JR, Gochuico B, Travis WD. Acute fibrous and organizing pneumonia. Arch Pathol Lab Med. 2002. 126:1064–1070.
2. American Thoracic Society and European Respiratody Society. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. Am J Respir Crit Care Med. 2002. 165:277–304.
3. Vourlekis JS, Brown KK, Schwart MI. Acute interstitial pneumonitis: current understanding regarding diagnosis, pathogenesis, and natural history. Semin Respir Crit Care Med. 2001. 22:399–408.
4. Yazdy AM, Tomashefski JF Jr, Yagan R, Kleinerman J. Regional alveolar damage (RAD): a localized counterpart of diffuse alveolar damage. Am J Clin Pathol. 1989. 92:10–15.
5. Lamy M, Fallat RJ, Koeniger E, Dietrich HP, Ratliff JL, Eberhart RC, et al. Pathologic features and mechanisms of hypoxemia in adult respiratory distress syndrome. Am Rev Respir Dis. 1976. 114:267–284.
6. Tomashefski JF Jr. Pulmonary pathology of the adult respiratory distress syndrome. Clin Chest Med. 1990. 11:593–619.
7. Tazelaar HD, Linz LJ, Colby TV, Myers JL, Limper AH. Acute eosinophilic pneumonia: histopathologic findings in nine patients. Am J Respir Crit Care Med. 1997. 155:296–302.
8. Muller NL, Guerry-Force ML, Staples CA, Wright JL, Wiggs B, Coppin C, et al. Differential diagnosis of bronchiolitis obliterans with organizing pneumonia and usual interstitial pneumonia: clinical, functional, and radiologic findings. Radiology. 1987. 162:151–156.
9. Savici D, Katzenstein AL. Diffuse alveolar damage and recurrent respiratory failure: report of six cases. Hum Pathol. 2001. 32:1398–1402.
10. Vourlekis JS, Brown KK, Schwarz MI. Acute interstitial pneumonitis: current understanding regarding diagnosis, pathogenesis, and natural history. Semin Respir Crit Care Med. 2001. 22:399–408.
11. Muller NL, Colby TV. Idiopathic interstitial pneumonias: high-resolution CT and histologic findings. Radiographics. 1997. 17:1016–1022.
12. Katzenstein AL, Myers JL, Mazur MT. Acute interstitial pneumonia: a clinico-pathologic, ultrastructural, and cell kinetic study. Am J Surg Pathol. 1986. 10:256–267.
13. Bouros D, Nicholson AC, Polychronopoulos V, du Bois RM. Acute interstitial pneumonia. Eur Respir J. 2000. 15:412–418.
14. Kobayshi H, Itoh T, Sasaki Y, Konishi J. Diagnostic imaging of idiopathic adult respiratory distress syndrome (ARDS)/ diffuse alveolar damage (DAD): histopathological correlation with radiological imaging. Clin Imaging. 1996. 20:1–7.
 XML Download
XML Download