

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Diffuse infiltrative lymphocytosis syndrome is an autoimmune syndrome that is characterized by the oligoclonal expansion of CD8+ T-lymphocytes in response to human immunodeficiency virus (HIV) antigens. The clinical manifestations include bilateral enlargement of the parotid glands, lymphocytic interstitial pneumonitis, lymphocytic hepatitis, neurological involvement and systemic lymphadenopathies. In addition to a positive HIV test, the diagnostic histopathological findings are CD8+ T-lymphocytic infiltrations in the lymphnodes, liver, lung, muscle and the salivary or lacrimal glands without granulomatous or neoplastic involvement. We report a case of pulmonary involvement of diffuse infiltrative lymphocytosis syndrome that was associated with a human immunodeficiency virus infection.
Figures and Tables
Figure 1
Chest X-ray. Diffuse bilateral mixed fine reticular and poorly-defined micronodular opacities are distributed at both lung fields.

Figure 2
High Resolution Computed Tomography of lung on admission. Mixed fine and poorly defined micronodules are scattered at both lung fields. Centrilobobular micronodules are distributed in both lung fields.

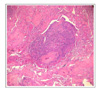
Figure 3
Excisional biopsy of mucosal polyp at lower lip (H&E staining, ×400). Acanthosis, parakeratosis, and intracellular edema associated with characteristic nuclear inclusions are consistent with hairy leukoplakia of HIV-infected individual.
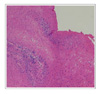
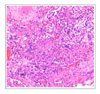
Figure 4
Open surgical lung biopsy (H&E staining, ×40). Diffuse and nodular infiltrations of interstitial lymphoplasma cells are revealed in peri-bronchiolar and peri-vascular spaces.

References
1. Brugnoni D, Prati E, Malacarne F, Gorla R, Airo P, Cattaneo R. The primary response to HIV infection is characterized by an expasion of activated CD8+ CD28-cells. AIDS. 1996. 10:104–106.
2. Roos MT, Lange JM, de Geode RE, Coultinho RA, Schellekens PT, Miedema F, et al. Viral phenotype and immune response in primary human immunodeficiency virus type 1 (HIV-1) infection. J Infect Dis. 1992. 165:427–432.
3. Livingstone WJ, Moore M, Innes D, Bell JE, Simmonds P. Frequent infection of peripheral blood CD8-positive T-lymphocytes with HIV-1. Lancet. 1996. 348:649–654.
4. Itescu S, Bracato LJ, Buxbaum J, Gregersen PK, Rizk CC, Croxson TS, et al. A diffuse infiltrative lymphocytosis syndrome in human immunodeficiency virus (HIV) infection: a host immune response associated with HLA-DR5. Ann Intern Med. 1990. 112:3–10.
5. Kazi S, Cohen PR, Williams F, Schempp R, Reveille JD. The diffuse infiltrative lymphocytosis syndrome: clinical and immunogenetic features in 35 patients. AIDS. 1996. 10:385–391.
6. Moulignier A, Authier FJ, Baudrimont M, Pialoux G, Belec L, Polivka M, et al. Peripheral neuropathy in human immunodeficiency virus-infected patients with the diffuse infiltrative lymphocytosis syndrome. Ann Neurol. 1997. 41:438–445.
7. Solal-Celigny P, Couderc LJ, Herman D, Herve P, Schaffar-Desha-yes L, Brun-Vezinet F, et al. Lymphoid interstitial pneumonitis in acquired immunodeficiency syndrome-related complex. Am Rev Respir Dis. 1985. 131:956–960.
8. Kordossis T, Paikos S, Aroni K, Kitsanta P, Dimitrakopoulos A, Kavouklis E, et al. Prevalence of Sjogren's-like syndrome in a cohort of HIV-1 positive patients: descriptive pathology and immunopathology. Br J Rheumatol. 1998. 37:691–695.
9. Williams FM, Cohen PR, Jumshyd J, Revrille JD. Prevalence of the diffuse infiltrative lymphocytosis syndrome among human immunodeficiency virus type-1 positive outpatients. Arthritis Rheum. 1998. 41:863–868.
10. Itescu S, Winchester R. Diffuse infiltrative lymphocytosis syndrome: a disorder occurring in human immunodeficiency virus-1 infection that may present as a sicca syndrome. Rheum Dis Clin North Am. 1992. 18:683–697.
11. Adamson TC 3rd, Fox RI, Frisman DM, Howell FV. Immunohistologic analysis of lymphoid infiltrates in primary Sjogren's syndrome using monoclonal antibodies. J Immunol. 1983. 130:203–208.
12. Mann DL, Moutsopoulos HM. HLA-DR5 alloantigens in different subsets of patients with Sjogren's syndrome and in family members. Ann Rheum Dis. 1983. 42:533–536.
13. Moutsopoulos HM, Chused TM, Mann DL, Kilppel JH, Fauci AS, Frank MM, et al. Sjogren's syndrome (sicca syndrome): current issues. Ann Intern Med. 1980. 92:212–226.
14. Meybeck A, Breton G, Aoun N, Able-Biassette H, Jacobelli S, Vilde JL, et al. Upper respiratory tract involvement in the course of diffuse infiltrative lymphocytosis syndrome in HIV-1 infected patients: report of 2 cases. Clin Infect Dis. 2005. 41:22–26.
 XML Download
XML Download