

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Cervical tuberculous lymphadenopathy is a very common disease with a similar incidence to pulmonary tuberculosis. Dendritic cells play a role of initial antigen presentation of this illness. Nevertheless, the precise role of these antigen-presenting cells according to the clinical features in unclear. The aim of this study was to determine the clinical implication of dendritic cell infiltration in the cervical lymph nodes.
Methods
A review of the clinical characteristics was carried out retrospectively based on the clinical records and radiography. Immunohistochemical staining was performed on the available histology specimens of 72 cases using the S-100b polyclonal antibody for dendritic cells. The number of dendritic cells with tuberculous granuloma were determined. A X2 test, unpaired T test and multiple logistic regression analysis were performed.
Results
Thirty percent of subjects had previous or concurrent pulmonary TB. Twenty one percent of cases showed a positive reaction on the AFB stain. Within a granuloma, the number of infiltrated dendritic cells was 113.0±7.0. The incidence of fever and cough decreased with increasing infiltration of dendritic cells Multivariate regression analysis showed that the infiltration of dendritic cells could significantly contribute to fever.
Figures and Tables
 | Figure 1Hypothetical scheme for tuberculosis in the lungs and lymph node.
M. tuberculosis, Mycobacterium tuberculosis; DC, dendritic cells; MHC, major histocompatibility complex
In pulmonary tuberculosis, dendritic cells have role of initial antigen presentation.
|
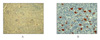


Table 3
Comparison of clinical & microscopic characteristics between abscess positive and abscess negative group

![]()
Table 4
Comparison of clinical & microscopic characteristics between fever positive and fever negative group

![]()


References
1. Ministry of Health & Welfare. The Korean National Tuberculosis Association. The fifth nationwide tuberculosis prevalence survey in Korea. 1985.
2. Han YS, Jeoung JW, Park SH, Byun HW. A clinical study on organ distribution of tuberculosis. Tuberc Respir Dis. 1979. 26:15–20.
3. Nararng P, Narang R, Mendiratta DK, Sharma SM, Tyagi NK. Prevalence of tuberculous lymphadenitis in children in Wardha district, Maharashtra State, India. Int J Tuberc Lung Dis. 2005. 9:188–194.
4. Park HJ, Ryoo HM, Shin KC, Park JS, Chung JH, Lee KH, et al. A clinical study of tuberculous lymphadenitis. Tuberc Respir Dis. 2000. 48:730–739.
5. Schlossberg D. Dwight a powell. Tuberculosis. 1993. 143.
6. Lew WJ, Lim BS, Choi WY, Shin DH, Park SS, Lee JH. Clinical analysis of 306 cases of cervical lymphadenopathy. Tuberc Respir Dis. 1991. 38:45–52.
7. Lipscomb FM, Masten JB. Dendritic cells: immune regulators in health and disease. Physiol Rev. 2002. 82:97–130.
8. Marino S, Kirschner DE. The human immune response to Mycobacterium tuberculosis in lung and lymph node. J Theor Biol. 2004. 227:463–486.
9. Austyn JM. Antigen-presenting cells: exterimental and clinical studies of dendritic cells. Am J Respir Crit Care Med. 2000. 162:S146–S150.
10. Bhatt K, Hickmen SP, Salgame P. A new approach to modeling early lung immunity in murine tuberculosis. J Immunol. 2004. 172:2748–2751.
11. Marino S, Pawar S, Fuller CL, Reinhart TA, Flynn JL, Kirschner DE. Dedritic cell trafficking and antigen presentation in the human immune respones to Mycobacterium tuberculosis. J Immunol. 2004. 173:494–506.
12. Schless JM, Wier JA. The current status and treatment of lymphatic tuberculosis. Am Rev Tuberc. 1957. 76:811–831.
13. Murty TV. Tuberculous lymphadenitis in children. Indian Pediatr. 1976. 13:533–538.
14. Thorek P. Surgical diagnosis. 1965. 2nd ed. Philadelphia: Lippicott.
15. Ahn CM, Kim HJ, Yoo KH, Park KJ, Kim SK, Lee WY. Clinical features in primary mediastinal tuberculous lymphadenitis. Tuberc Respir Dis. 1999. 46:767–774.
16. Gonzales-Juarrero M, Orme IM. Characterization of murine lung dendritic cells infected with Mycobacterium tuberculosis. Infect Immun. 2001. 69:1127–1133.
17. Engering A, Geijtenbeej TB, van Vliet SJ, Wijers M, van Liempt E, Demaurex N, et al. The dendritic cell-specific adhesion receptor DC-SIGN internalizes antigen for presentation to T cells. J Immunol. 2002. 168:2118–2126.
18. Mahnke K, Guo M, Le S, Sepulveda H, Swain SL, Nusenzweig M, et al. The dendritic cell receptor for endocytosis, DEC-205, can recycle and enhance antigen presentation via MHC II, lysosomal compartment. J Cell Biol. 2000. 151:673–684.
 XML Download
XML Download