

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Acute exacerbations form a major component of the socioeconomic burden of COPD. As yet, little information is available about the long-term outcome of patients who have been hospitalized with acute exacerbations, although high mortality rates have been reported. The aim of this study was to determine predictors of long-term mortality after hospitalization for acute exacerbation of COPD.
Methods
We performed a retrospective cohort study of consecutive patients admitted to the hospital for COPD exacerbation between 2000 through 2004. Patients who had died in hospital or within 6-months after discharge, had tuberculosis scar, pleural thickening or bronchiectasis by chest radiography or had been diagnosed with malignancy during follow-up periods were excluded.
Results
Mean age of patients was 69.5 years, mean follow-up duration was 49 months, and mean FEV1 was 1.00L (46% of predicted). Mortality was 35% (17/48). In the multivariate Cox regression analysis, heart rate of 100/min or more (p=0.003; relative risk [RR], 11.99; 95% confidence interval [CI], 2.34-61.44) and right ventricular systolic pressure (RVSP) of 35mmHg or more (p=0.019; RR, 6.85; 95% CI, 1.38-34.02) were independent predictors of mortality.
Figures and Tables

Figure 2
Survival curve during follow-up for the presence or absence of tachycardia in stable state of COPD.
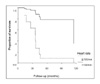
Figure 3
Survival curve during follow-up for different levels of right ventricular systolic pressure (RVSP) measured using echocardiography.
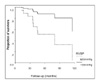




Table 5
Lung function in survivors and non-survivors with COPD in stable state*

NS, not significant; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity.
*Data are number (%) or mean±SD.
†Global initiative for chronic Obstructive Lung Disease (GOLD) criteria as follows: mild, FEV1≥80% of predicted; moderate, 50%≤FEV1<80%; severe, 30%≤ FEV1< 50%; very severe, FEV1<30%



References
1. Mannino DM. COPD: epidemiology, prevalence, morbidity and mortality, and disease heterogeneity. Chest. 2002. 121:Suppl. 121S–126S.
2. Yun SH. Acute exacerbation of chronic obstructive pulmonary disease. Korean J Crit Care Med. 2003. 18:1–6.
3. Patil SP, Krishnan JA, Lechtzin N, Diette GB. In-hospital mortality following acute exacerbations of chronic obstructive pulmonary disease. Arch Intern Med. 2003. 163:1180–1186.
4. Almagro P, Calbo E, Ochoa de Echaguen A, Barreiro B, Quintana S, Heredia JL, et al. Mortality after hospitalization for COPD. Chest. 2002. 121:1441–1448.
5. Anthonisen NR, Wright EC, Hodgkin JE. Prognosis in chronic obstructive pulmonary disease. Am Rev Respir Dis. 1986. 133:14–20.
6. Connors AF Jr, Dawson NV, Thomas C, Harrell FE Jr, Desbiens N, Fulkerson WJ, et al. Outcomes following acute exacerbation of severe chronic obstructive lung disease: the SUPPORT investigators (Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments). Am J Respir Crit Care Med. 1996. 154:959–967.
7. Groenewegen KH, Schols AM, Wouters EF. Mortality and mortality-related factors after hospitalization for acute exacerbation of COPD. Chest. 2003. 124:459–467.
8. Hansen EF, Phanareth K, Laursen LC, Kok-Jensen A, Dirksen A. Reversible and irreversible airflow obstruction as predictors of overall mortality in asthma and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999. 159:1267–1271.
9. Traver GA, Cline MG, Burrows B. Predictors of mortality in chronic obstructive pulmonary disease: a 15-year follow-up study. Am Rev Respir Dis. 1979. 119:895–902.
10. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACH II: a severity of disease classification system. Crit Care Med. 1985. 13:818–829.
11. Ai-Ping C, Lee KH, Lim TK. In-hospital and 5-year mortality of patients treated in the ICU for acute exacerbation of COPD: a retrospective study. Chest. 2005. 128:518–524.
12. Goel A, Pinckney RG, Littenberg B. APACHE II predicts long-term survival in COPD patients admitted to a general medical ward. J Gen Intern Med. 2003. 18:824–830.
13. Nevins ML, Epstein SK. Predictors of outcome for patients with COPD requiring invasive mechanical ventilation. Chest. 2001. 119:1840–1849.
14. Fuso L, Incalzi RA, Pistelli R, Muzzolon R, Valente S, Pagliari G, et al. Predicting mortality of patients hospitalized for acutely exacerbated chronic obstructive pulmonary disease. Am J Med. 1995. 98:272–277.
15. Standards for the diagnosis and management of patients with COPD [Internet]. Version 1.2. American Thoracic Society/European Respiratory Society Task Force. 2004. updated 2005 September 8. New York: American Thoracic Society;
http://www.thoracic.org/copd/.
16. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001. 163:1256–1276.
17. American Thoracic Society. Standardization of spirometry: 1994 update. Am J Respir Crit Care Med. 1995. 152:1107–1136.
18. Feigenbaum H, Armstrong WF, Ryan T. Feigenbaum's echocardiography. 2005. 6th ed. London: Lippincott Williams & Wilkins.
19. Seneff MG, Wagner DP, Wagner RP, Zimmerman JE, Knaus WA. Hospital and 1-year survival of patients admitted to intensive care units with acute exacerbation of chronic obstructive pulmonary disease. JAMA. 1995. 274:1852–1857.
20. Dallari R, Barozzi G, Pinelli G, Meright V, Grandi P, Manzotti M, et al. Predictors of survival in subjects with chronic obstructive pulmonary disease treated with long-term oxygen therapy. Respiration. 1994. 61:8–13.
21. Skwarski K, MacNee W, Wraith PK, Silwinski P, Zielinski J. Predictors of survival in patients with chronic obstructive pulmonary disease treated with long-term oxygen therapy. Chest. 1991. 100:1522–1527.
22. Wuertemberger G, Zielinsky J, Sliwinsky P, Auw-Haedrich C, Matthys H. Survival in chronic obstructive pulmonary disease after diagnosis of pulmonary hypertension related to long-term oxygen therapy. Lung. 1990. 168:762–769.
23. Boussuges A, Pinet C, Molenat F, Burnet H, Ambrosi P, Badier M, et al. Left atrial and ventricular filling in chronic obstructive pulmonary disease: an echocardiography and doppler study. Am J Respir Crit Care Med. 2000. 162:670–675.
24. Lacasse M, Maltais F, Poirier P, Lacasse Y, Marquis K, Jobin J, et al. Post-exercise heart rate recovery and mortality in chronic obstructive pulmonary disease. Respir Med. 2005. 99:877–886.
25. Burrows B, Earle RH. Prediction of survival in patients with chronic airway obstruction. Am Rev Respir Dis. 1969. 99:865–871.
26. Landbo C, Prescott E, Lange P, Vestbo J, Almdal TP. Prognostic value of nutritional status in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999. 160:1856–1861.
27. Celli BR, Cote CG, Marin JM, Casanova C, Montes de Oca M, Mendez RA, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004. 350:1005–1012.
28. Chailleux E, Laaban JP, Veale D. Prognostic value of nutritional depletion in patients with COPD treated by long-term oxygen therapy: data from the ANTADIR observatory. Chest. 2003. 123:1460–1466.
29. Fuld JP, Kilduff LP, Neder JA, Pitsiladis Y, Lean ME, Ward SA, et al. Creatine supplementation during pulmonary rehabilitation in chronic obstructive pulmonary disease. Thorax. 2005. 60:531–537.
30. Schols AM, Wesseling G, Kester AD, de Vries G, Mostert R, Slangen J, et al. Dose dependent increased mortality risk in COPD patients treated with oral glucocorticoids. Eur Respir J. 2001. 17:337–42.
 XML Download
XML Download