

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastric cancer (GC) is the second leading cause of cancer-related mortality and the fourth most commonly diagnosed malignant disease, with an estimated 740,000 cancer-related deaths and 990,000 new cases annually [12]. The prevalence of GC shows large regional variations [3]. The incidence of GC has decreased in the United States over the past 80 years. However, GC in South Korea accounts for approximately 17% of all prevalent cancer cases and about 12% of all cancer-related mortalities (nearly 9,000 deaths) annually [4]. The complete surgical resection of localized GC with the removal of adjacent lymph nodes is the only curative option, and patients with pathological stage II or III GC are recommended adjuvant therapy in addition to surgery [5]. The Adjuvant Chemotherapy Trial of TS-1 for Gastric Cancer (ACTS-GC) and the Capecitabine and Oxaliplatin Adjuvant Study in Stomach Cancer (CLASSIC) trial have demonstrated survival benefits of adjuvant therapy after D2 dissection surgery [67]. Unfortunately, due to the asymptomatic early phase of the disease, many patients with GC are diagnosed in advanced stages. Several phase III trials utilizing target-specific agents for inoperable and advanced GC have been conducted with very few favorable outcomes, specifically with trastuzumab (human epidermal growth factor receptor 2 [HER2]-targeted monoclonal antibody) [8], ramucirumab (vascular endothelial growth factor receptor 2 [VEGFR2]-targeted monoclonal antibody) [9], and apatinib (VEGFR2-targeted tyrosine kinase inhibitor [TKI]) [10]. Therefore, advances made to increase the survival rate of patients suffering from GC have been much slower than those concerned with other cancers over the past decade.
GC is considered as a heterogeneous disease carrying various genetic mutations [11]. While satisfactory results were expected from various target-specific agents, most of the trials with these agents were failures. The one-size-fits-all approach to treatment is considered a key reason for the failure of these trials, and patient selection based on appropriate biomarkers is essential for successful trials [12].
In this article, we review target-specific agents currently used in clinics or are undergoing clinical trials, and highlight the future clinical application of immuno-oncologic agents in inoperable GC.
ErbB FAMILY-TARGETING AGENTS
The HER2 protein is a member of the ErbB family comprising 4 kinds of receptor tyrosine kinases (RTKs). The ErbB family of proteins includes transmembrane receptors composed of an intracellular region with a tyrosine kinase residue, an extracellular ligand-binding domain, and a single hydrophobic transmembrane segment. The HER2 protein plays a crucial role in cancer cell biology [13], and mediates apoptosis, cellular differentiation, and tumorigenesis [14]. Compared with other members of the ErbB family, HER2 lacks an identifiable ligand. The ligand-free activation of the HER2 receptor occurs via hetero- or homo-dimerization with other ErbB family members, resulting in the upregulation of downstream signaling cascades, including RAS-RAF-mitogen-activated protein kinase (MAPK), MAPK-extracellular signal-regulated kinase (MEK), and phosphatidylinositol 3-kinase (PI3K)-Akt-mammalian target of rapamycin (mTOR) pathways [1516]. HER2 gene amplification has been reported in about 15%–30% of patients with breast cancer, and is associated with poor prognosis [1718]. Its amplification also occurs in GC (approximately 7%–34% of patients), ovarian cancer, non-small cell lung cancer, endometrial carcinoma, and salivary cancer [19202122].
Trastuzumab
Trastuzumab, a monoclonal antibody specifically targeting the extracellular domain of the HER2 protein, is reported to show remarkable antitumor activity in HER2-amplified xenograft models of human GC cell lines [23]. Based on these results, a randomized phase III Trastuzumab for Gastric Cancer (ToGA) trial was conducted as the first study demonstrating the efficacy of a target-specific agent in patients with advanced or metastatic GC [8]. The ToGA study enrolled patients treated with first-line palliative chemotherapy. In this trial, 3,803 patients were evaluated for HER2 status by immunohistochemistry (IHC) as well as fluorescence in situ hybridization (FISH), and 594 patients who showed 3+ on IHC or FISH positivity (HER2: centromeric probe for chromosome 17 [CEP17] ratio ≥2) were randomly assigned to receive chemotherapy (fluoropyrimidine+cisplatin) with or without trastuzumab. The median overall survival (OS) in patients who underwent chemotherapy+trastuzumab was 13.8 months (95% confidence interval [CI], 12–16) compared with 11.1 months (95% CI, 10–13) in patients who underwent chemotherapy alone (hazard ratio [HR], 0.74; 95% CI, 0.60–0.91; P=0.005). The median progression-free survival (PFS) in patients who received chemotherapy+trastuzumab was 6.7 months (95% CI, 6–8) compared with 5.5 months (95% CI, 5–6) in the other group (HR, 0.71; 95% CI, 0.59–0.85; P<0.001). In post hoc analyses, no improvement in OS with trastuzumab was observed in patients with HER2 IHC0/FISH+ or IHC1+/FISH+, while significant improvement in OS was observed in patients with HER2 IHC2+/FISH+ or IHC3+. In cases of HER2 IHC scores of 0, 1+, or 3+, the concordance rate with FISH results exceeded 85%; however, the concordance rate with FISH results in the case of IHC2+ was only about 50%, suggesting that additional FISH tests were mandatory to determine HER2 expression levels [24]. Following the promising results of the ToGA trial in 2010, the Food and Drug Administration (FDA) approved trastuzumab for chemo-naïve HER2-overexpressing metastatic GC.
Pertuzumab
Pertuzumab is a monoclonal antibody inhibiting dimerization by targeting the HER2 ectodomain [25]. The combination of trastuzumab with pertuzumab showed superior antitumor activities compared with the individual drugs in HER2-overexpressing xenograft models of human GC [26] as well as HER2-overexpressing metastatic breast cancer [27]. A phase III study designated as the JACOB trial involved patients who were randomized to receive pertuzumab or placebo in combination with trastuzumab, cisplatin, and fluoropyrimidine. This study was conducted to evaluate the efficacy of pertuzumab in addition to survival benefits observed in the ToGA trial with the first-line treatment of HER2-positive metastatic GC. However, according to the results reported at the 2017 European Society for Medical Oncology Congress, the JACOB study failed to show a significant improvement in OS with the addition of pertuzumab, despite a 3.3-month increase in median OS (NCT01774786).
TKIs targeting HER2
Lapatinib, a small-molecule TKI targeting HER2 and epidermal growth factor receptor (EGFR), showed favorable clinical results in patients with HER2-positive metastatic breast cancer in a phase III, randomized, open-label study as well as in a meta-analysis report [2829], and the FDA approved this drug in trastuzumab-resistant breast cancer patients. However, 2 phase III clinical trials conducted in GC patients were unsuccessful. In the phase III LOGiC trial, which enrolled 545 patients with HER2-positive GC, participants were randomized to receive capecitabine+oxaliplatin (CapeOx) with or without lapatinib as the first-line regimen. There was no significant benefit in OS (HR, 0.91; 95% CI, 0.73–1.12; P=0.350) [30]. In the phase III TyTAN study, lapatinib was evaluated as a second-line treatment in HER2-positive GC. Participants in this trial were randomized to receive paclitaxel treatment with or without lapatinib. No significant improvement in OS was observed (HR, 0.84; 95% CI, 0.64–1.11; P=0.104) [31].
Afatinib, another TKI targeting EGFR, HER2, and HER4 was approved by the FDA for the treatment of non-small cell lung cancer bearing EGFR mutations. Based on a preclinical study demonstrating tumor regression by afatinib treatment in HER2-amplified GC cell xenograft models [32], 3 phase II trials of afatinib in GC are ongoing (NCT02501603, NCT01522768, and NCT01743365).
Trastuzumab-emtansine (T-DM1)
T-DM1 is a monoclonal antibody-microtubule inhibitor (maytansine) conjugate exhibiting both cytotoxic properties and antibody-dependent cytotoxicity [33]. T-DM1 exerted beneficial effects in patients with HER2-amplified metastatic breast cancer [34], and preclinical data indicated that T-DM1 is more efficacious than trastuzumab alone in GC cell xenograft models [35]. Given these results, a phase II/III trial of T-DM1, GATSBY (NCT01641939), was conducted in locally advanced or metastatic HER2-positive GC patients who exhibited disease progression following first-line treatment; however, T-DM1 did not improve OS compared with taxane (HR, 1.15; 95% CI, 0.89–1.43; P=0.860) [36].
Agents targeting EGFR
Agents targeting EGFR have been used as a standard treatment for many cancers, including colorectal cancer, non-small cell lung cancer, pancreatic cancer, breast cancer, and head & neck cancer. Anti-EGFR agents include cetuximab, panitumumab, nimotuzumab, gefitinib, and erlotinib. Since EGFR overexpression was observed in GC, which was shown to be associated with poor prognosis [3738], several trials investigating EGFR as a target for the treatment of GC were conducted.
Nevertheless, despite several favorable phase II results [3940414243], a phase III trial of cetuximab as first-line treatment (EXPAND) failed to reach the primary end point (HR, 1.09; 95% CI, 0.92–1.29; P=0.320) [44].
A phase III trial of panitumumab as first-line treatment (REAL3) reduced OS (HR, 1.37; 95% CI, 1.07–0.76; P=0.013) [45]. A phase III study of the efficacy of nimotuzumab as second-line treatment in advanced or recurrent GC was prematurely terminated because of the lack of a positive outcome in the mid-term follow-up (NCT01813253, ENRICH).
ANTI-ANGIOGENESIS
Angiogenesis is a mechanism of neovascularization from previously existing vessels known to promote carcinogenesis and cancer metastasis [4647]. VEGF gene family proteins, including VEGFA, B, C, and D, and placental growth factor are signal proteins that induce angiogenesis and lymphangiogenesis [48]. Receptors of this gene family, designated as VEGFR1, R2, and R3, are types of RTKs usually expressed in lymphatic or vascular endothelial (VE) cells [46]. Among these receptors, VEGFR2 is the main effector of RTK and mediates downstream signaling cascades, including the phospholipase C-γ-protein kinase C-MEK-MAPK pathway and PI3K-Akt-endothelial nitric oxide synthase pathway [464950]. VEGF overexpression is frequently found in GC patients and is closely associated with poor clinical outcomes [51].
Bevacizumab
Bevacizumab is a monoclonal antibody targeting VEGFA and is approved by the FDA for the treatment of colorectal cancer. In the phase III Avastin in Gastric Cancer (AVAGAST) trial, 774 patients with GC were randomized to receive fluoropyrimidine+cisplatin with bevacizumab or placebo as first-line treatment [52]. In terms of OS, there was no significant difference between the 2 groups (HR, 0.87; 95% CI, 0.73–1.03; P=0.100). However, bevacizumab was efficacious in terms of PFS (HR, 0.80; 95% CI, 0.68–0.93; P=0.004) and overall response rate (ORR) (46% vs. 37%; P=0.032). Strangely, results of this study showed a geographical variation; OS significantly improved with bevacizumab in Europe and America, but not in Asia. One of the reasons for failure in Asia is that the efficacy of bevacizumab as first-line treatment in OS was compromised as many patients in Asia receive second-line and additional treatments. Another phase III trial on bevacizumab (AVATAR), which was conducted in China, also failed to show an improvement in OS (HR, 1.11; 95% CI, 0.79–1.56; P=0.557) [53].
Ramucirumab
The efficacy of ramucirumab, a monoclonal antibody targeting VEGFR2 [54], has been investigated as second-line treatment for GC patients in 2 phase III trials (REGARD and RAINBOW) [955]. In the REGARD trial, a slight improvement in OS was obtained by ramucirumab monotherapy compared with placebo, validating VEGFR2 as a crucial target in GC (HR, 0.77; 95% CI, 0.60–0.99; P=0.047). In the subsequent RAINBOW trial, 665 GC patients who failed to respond to first-line chemotherapy, including fluoropyrimidine and platinum, were randomized to receive ramucirumab+paclitaxel or placebo+paclitaxel treatment. OS was significantly longer in the paclitaxel+ramucirumab group than in the placebo+paclitaxel group (HR, 0.80; 95% CI, 0.67–0.96; P=0.017), and the FDA approved ramucirumab in GC patients exhibiting disease progression with first-line treatment. As a result, a phase III trial evaluating the efficacy of ramucirumab as first-line treatment in metastatic GC is ongoing (NCT02314117, RAINFALL).
TKIs targeting VEGFR2
Apatinib is a small-molecule TKI inhibiting VEGFR2 tyrosine kinase. In a multicenter phase III trial conducted in China, GC patients who were refractory to at least 2 prior lines of standard chemotherapies were randomized to receive apatinib or placebo [10]. OS significantly increased in the apatinib group (HR, 0.71; 95% CI, 0.54–0.94; P<0.016), and apatinib was approved only in China. Another multicenter phase III study investigating apatinib efficacy in advanced or metastatic GC patients who were refractory to at least 2 prior treatments is ongoing (NCT03042611, ANGEL).
Regorafenib is an oral multi-kinase inhibitor, which blocks angiogenic (VEGFR2 and endothelial-specific type 2), stromal (platelet-derived growth factor-β), and oncogenic (RAF, RET, and KIT) RTKs. Regorafenib has been proven effective in GC cell xenograft models [56] and in a phase II trial (HR, 0.40; 95% CI, 0.28–0.59; P<0.001) [57]. Based on these results, a multicenter phase III trial of regorafenib efficacy in refractory advanced GC is ongoing (NCT02773524, INTEGRATEII).
OTHER TARGET-SPECIFIC AGENTS
The protein c-MET, an RTK regulating cell proliferation and invasion, and its ligand, hepatocyte growth factor (HGF), activates downstream signaling cascades, including MAPK and PI3K-Akt pathways. MET gene amplification is observed in about 10%–20% of GC patients, and increased MET protein expression is observed in approximately 50% of GC patients [5859]. Furthermore, in a phase Ib/II trial, rilotumumab, an anti-HGF antibody was shown to be effective in MET-positive GC patients [60]. However, 2 phase III trials of rilotumumab (RILOMET-1 and RILOMET-2) failed to reach the primary endpoint [6162]. A phase III study of onartuzumab, a monoclonal antibody targeting c-MET, also failed to improve OS [63].
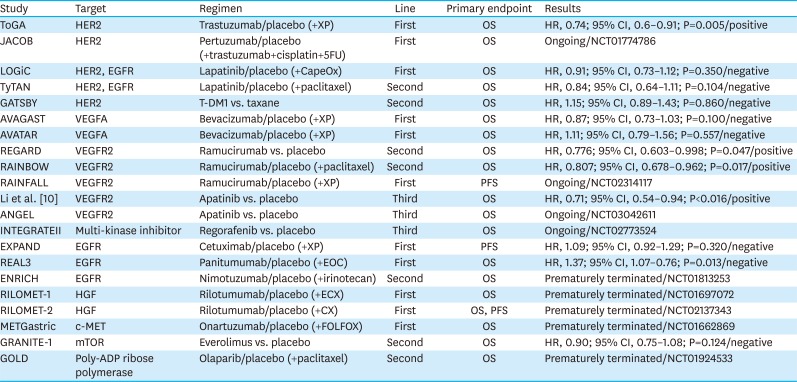
The mTOR inhibitor everolimus was shown to be effective in GC patients in a phase II study; however, a phase III study (GRANITE-1) of this drug failed to show efficacy [6465]. The combination of a TKI targeting fibroblast growth factor receptor (FGFR) 1–3, AZD4547, and paclitaxel also lacked efficacy as the second-line treatment of FGFR2-amplified GC in a phase II trial (SHINE) [66]. A poly-ADP ribose polymerase inhibitor, olaparib, was evaluated as a treatment for advanced GC in a phase III trial (NCT01924533, GOLD), but failed to show efficacy [67]. Phase III randomized clinical trials with target-specific agents are summarized in Table 1.
Table 1
Phase III randomized clinical trials of targeted therapies
| Study | Target | Regimen | Line | Primary endpoint | Results |
|---|---|---|---|---|---|
| ToGA | HER2 | Trastuzumab/placebo (+XP) | First | OS | HR, 0.74; 95% CI, 0.6–0.91; P=0.005/positive |
| JACOB | HER2 | Pertuzumab/placebo (+trastuzumab+cisplatin+5FU) | First | OS | Ongoing/NCT01774786 |
| LOGiC | HER2, EGFR | Lapatinib/placebo (+CapeOx) | First | OS | HR, 0.91; 95% CI, 0.73–1.12; P=0.350/negative |
| TyTAN | HER2, EGFR | Lapatinib/placebo (+paclitaxel) | Second | OS | HR, 0.84; 95% CI, 0.64–1.11; P=0.104/negative |
| GATSBY | HER2 | T-DM1 vs. taxane | Second | OS | HR, 1.15; 95% CI, 0.89–1.43; P=0.860/negative |
| AVAGAST | VEGFA | Bevacizumab/placebo (+XP) | First | OS | HR, 0.87; 95% CI, 0.73–1.03; P=0.100/negative |
| AVATAR | VEGFA | Bevacizumab/placebo (+XP) | First | OS | HR, 1.11; 95% CI, 0.79–1.56; P=0.557/negative |
| REGARD | VEGFR2 | Ramucirumab vs. placebo | Second | OS | HR, 0.776; 95% CI, 0.603–0.998; P=0.047/positive |
| RAINBOW | VEGFR2 | Ramucirumab/placebo (+paclitaxel) | Second | OS | HR, 0.807; 95% CI, 0.678–0.962; P=0.017/positive |
| RAINFALL | VEGFR2 | Ramucirumab/placebo (+XP) | First | PFS | Ongoing/NCT02314117 |
| Li et al. [10] | VEGFR2 | Apatinib vs. placebo | Third | OS | HR, 0.71; 95% CI, 0.54–0.94; P<0.016/positive |
| ANGEL | VEGFR2 | Apatinib vs. placebo | Third | OS | Ongoing/NCT03042611 |
| INTEGRATEII | Multi-kinase inhibitor | Regorafenib vs. placebo | Third | OS | Ongoing/NCT02773524 |
| EXPAND | EGFR | Cetuximab/placebo (+XP) | First | PFS | HR, 1.09; 95% CI, 0.92–1.29; P=0.320/negative |
| REAL3 | EGFR | Panitumumab/placebo (+EOC) | First | OS | HR, 1.37; 95% CI, 1.07–0.76; P=0.013/negative |
| ENRICH | EGFR | Nimotuzumab/placebo (+irinotecan) | Second | OS | Prematurely terminated/NCT01813253 |
| RILOMET-1 | HGF | Rilotumumab/placebo (+ECX) | First | OS | Prematurely terminated/NCT01697072 |
| RILOMET-2 | HGF | Rilotumumab/placebo (+CX) | First | OS, PFS | Prematurely terminated/NCT02137343 |
| METGastric | c-MET | Onartuzumab/placebo (+FOLFOX) | First | OS | Prematurely terminated/NCT01662869 |
| GRANITE-1 | mTOR | Everolimus vs. placebo | Second | OS | HR, 0.90; 95% CI, 0.75–1.08; P=0.124/negative |
| GOLD | Poly-ADP ribose polymerase | Olaparib/placebo (+paclitaxel) | Second | OS | Prematurely terminated/NCT01924533 |
HER2 = human epidermal growth factor receptor 2; XP = capecitabine+cisplatin; OS = overall survival; HR = hazard ratio; CI = confidence interval; 5FU = 5-fluorouracil; EGFR = epidermal growth factor receptor; CapeOx = capecitabine+oxaliplatin; T-DM1 = trastuzumab-emtansine; VEGFA = vascular endothelial growth factor A; VEGFR2 = vascular endothelial growth factor receptor 2; PFS = progression-free survival; EOC = epirubicin+oxaliplatin+capecitabine; HGF = hepatocyte growth factor; ECX = epirubicin+cisplatin+capecitabine; CX = cisplatin+capecitabine; FOLFOX = 5-fluorouracil+leucovorin+oxaliplatin; mTOR = mammalian target of rapamycin.
IMMUNOTHERAPY
A tumor cell is recognized by and is vulnerable to the host immune system. Classical reports of animal models have indicated that the immune system recognizes and eliminates tumor cells [68]. However, via elimination, equilibrium, and finally escape, cancer cells become invisible to the host [68]. Understanding the mechanism associated with immune escape led to the advancement of the field of immuno-oncology and the development of several target-specific agents, including anti-cytotoxic T-lymphocyte antigen 4 (CTLA-4) antibodies and programmed death-1 (PD-1)/programmed death-ligand 1 (PD-L1) inhibitors (Fig. 1).
Fig. 1
Immune checkpoint inhibitors and their targets, including ligands and receptors on tumor cells, T cells, and dendritic cell surfaces.
CTLA-4 = cytotoxic T-lymphocyte antigen 4; PD-1 = programmed death 1; PD-L1 = programmed death-ligand 1.
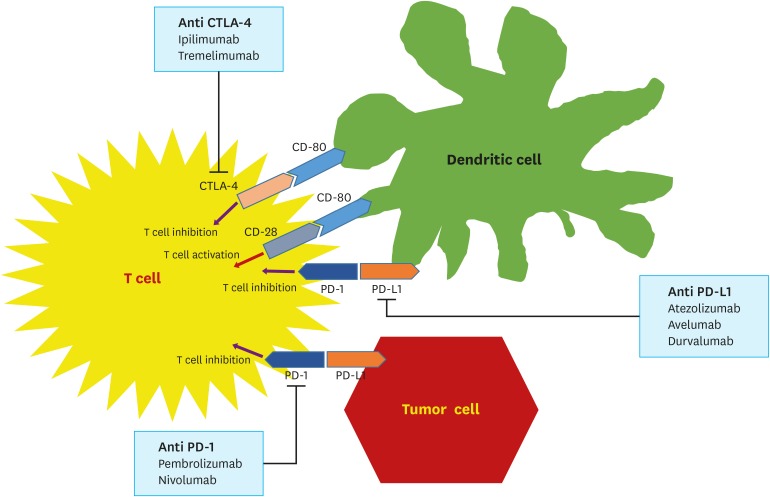
The activation of tumoricidal immune reactions requires the presentation of cancer antigens to T cells by either dendritic or cancer cells [69]. These interactions are regulated by a combination of co-stimulatory and inhibitory molecules [70]. CTLA-4 is an inhibitory receptor molecule expressed on cytotoxic T cells, and coordinates with CD80 or CD86 on antigen-presenting cells to suppress the cytotoxic activity of T cells. However, the binding of CD28, a co-stimulatory receptor on T cells, to CD80 or CD86 by competing with CTLA-4 increases the tumoricidal activity of T cells [71]. PD-1 is another inhibitory cell surface receptor expressed on antigen-specific CD8+ T cells; it binds to PD-L1 or PD-L2 on antigen-presenting cells to suppress host immune response, including T cell effector functions, migration, and proliferation [72]. Because PD-L1 is not only expressed on dendritic cells, macrophages, mast cells, and natural killer cells, it is also boosted by the cancer cell per se. Therefore, a PD-1/PD-L1 blockade is expected to enhance early immune reactions in lymphoid organs to late reactions at other locations [73].
For over a decade, the field of immuno-oncology has been in the spotlight owing to innovative practice-changing successes [74]. The therapeutic milestones involved melanomas, genitourinary cancers, lung cancers, and head & neck cancers. As a result, several trials on gastrointestinal cancers are ongoing.
Clinical trials of immune checkpoint inhibitors
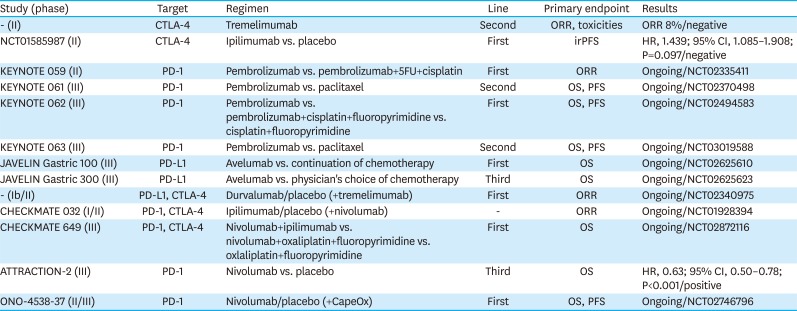
Clinical trials investigating immune checkpoint inhibitors are summarized in Table 2.
Table 2
Clinical trials investigating immune checkpoint inhibitors
| Study (phase) | Target | Regimen | Line | Primary endpoint | Results |
|---|---|---|---|---|---|
| - (II) | CTLA-4 | Tremelimumab | Second | ORR, toxicities | ORR 8%/negative |
| NCT01585987 (II) | CTLA-4 | Ipilimumab vs. placebo | First | irPFS | HR, 1.439; 95% CI, 1.085–1.908; P=0.097/negative |
| KEYNOTE 059 (II) | PD-1 | Pembrolizumab vs. pembrolizumab+5FU+cisplatin | First | ORR | Ongoing/NCT02335411 |
| KEYNOTE 061 (III) | PD-1 | Pembrolizumab vs. paclitaxel | Second | OS, PFS | Ongoing/NCT02370498 |
| KEYNOTE 062 (III) | PD-1 | Pembrolizumab vs. pembrolizumab+cisplatin+fluoropyrimidine vs. cisplatin+fluoropyrimidine | First | OS, PFS | Ongoing/NCT02494583 |
| KEYNOTE 063 (III) | PD-1 | Pembrolizumab vs. paclitaxel | Second | OS, PFS | Ongoing/NCT03019588 |
| JAVELIN Gastric 100 (III) | PD-L1 | Avelumab vs. continuation of chemotherapy | First | OS | Ongoing/NCT02625610 |
| JAVELIN Gastric 300 (III) | PD-L1 | Avelumab vs. physician's choice of chemotherapy | Third | OS | Ongoing/NCT02625623 |
| - (Ib/II) | PD-L1, CTLA-4 | Durvalumab/placebo (+tremelimumab) | First | ORR | Ongoing/NCT02340975 |
| CHECKMATE 032 (I/II) | PD-1, CTLA-4 | Ipilimumab/placebo (+nivolumab) | - | ORR | Ongoing/NCT01928394 |
| CHECKMATE 649 (III) | PD-1, CTLA-4 | Nivolumab+ipilimumab vs. nivolumab+oxaliplatin+fluoropyrimidine vs. oxlaliplatin+fluoropyrimidine | First | OS | Ongoing/NCT02872116 |
| ATTRACTION-2 (III) | PD-1 | Nivolumab vs. placebo | Third | OS | HR, 0.63; 95% CI, 0.50–0.78; P<0.001/positive |
| ONO-4538-37 (II/III) | PD-1 | Nivolumab/placebo (+CapeOx) | First | OS, PFS | Ongoing/NCT02746796 |
CTLA-4 = cytotoxic T-lymphocyte antigen 4; ORR = overall response rate; irPFS = immune-related progression-free survival; 5FU = 5-fluorouracil; HR = hazard ratio; CI = confidence interval; PD-1 = programmed death 1; OS = overall survival; PFS = progression-free survival; PD-L1 = programmed death-ligand 1; CapeOx = capecitabine+oxaliplatin.
The multicenter open-label phase Ib KEYNOTE 012 trial of pembrolizumab was conducted in several cancers, including GC, triple-negative breast cancer, head & neck cancer, and urothelial cancer. Out of 39 patients with GC included in this study, overall response was observed in 8 patients (22%; 95% CI, 10–39). Considering that most patients in this group had failed to respond to 2 or more prior treatments, the median OS of 11 months documented in this study was a remarkable result [75]. An international open-label phase II trial of pembrolizumab in 2 cohorts (patients who had failed to respond to 2 or more prior treatments and treatment-naïve patients) was performed, and the ORR was 13.3% (95% CI, 8.2–20.2) (NCT02335411, KEYNOTE 059). Based on the study findings, the FDA approved pembrolizumab for patients with PD-L1-positive recurrent or advanced GC, who previously received 2 or more chemotherapy regimens. There are 3 phase III, randomized, open-label trials of pembrolizumab, including KEYNOTE 061, KEYNOTE 062, and KEYNOTE 063 (NCT02370498, NCT02494583, and NCT03019588, respectively). KEYNOTE 061 trial investigated the efficacy of pembrolizumab versus paclitaxel as second-line treatment in patients with PD-L1-positive advanced GC who were refractory to fluoropyrimidine and platinum doublet therapy (NCT02370498). The KEYNOTE 062 trial, which investigated pembrolizumab as the first-line treatment, enrolled patients with HER2-negative, PD-L1-positive advanced GC, and randomly assigned participants into 3 treatment arms: pembrolizumab monotherapy, perbrolizumab+platinum+fluoropyrimidine, and placebo+platinum+fluoropyrimidine (NCT02494583). The KEYNOTE 063 trial compared the efficacy of treatment with pembrolizumab versus paclitaxel in Asian, PD-L1-positive patients with advanced GC who failed to respond to any combination treatment containing a fluoropyrimidine and a platinum agent (NCT03019588).
A phase I/II trial investigating the combination of an anti-PD-1 antibody nivolumab with an anti-CTLA-4 antibody ipilimumab in patients with advanced or metastatic solid tumors is underway (NCT01928394, CHECKMATE 032). A randomized, multicenter, open-label phase III trial of nivolumab+ipilimumab or nivolumab+oxaliplatin+fluoropyrimidine versus oxaliplatin+fluoropyrimidine in patients with treatment-naïve metastatic or advanced GC is also ongoing (NCT02872116, CHECKMATE 649).
The ATTRACTION-2 study was the first randomized, multicenter, double blind, phase III trial demonstrating the efficacy of immunotherapy in unresectable or recurrent GC patients [76]. In this study, 493 patients with GC refractory or intolerant to standard therapy were randomly assigned to receive nivolumab or placebo, and a significantly longer OS was observed in patients treated with nivolumab (HR, 0.63; 95% CI, 0.50–0.78; P<0.001). A randomized, multicenter, phase II/III trial comparing nivolumab+fluoropyrimidine+oxaliplatin versus placebo+fluoropyrimidine+oxaliplatin as first-line treatment for unresectable advanced or recurrent GC is ongoing (NCT02746796).
Potential predictive markers of immunotherapy in GC
Because of defects in DNA mismatch repair genes, cancers with microsatellite instability (MSI) possess a high number of mutations, and express numerous surface antigens for presentation to immune cells [77]. In recent studies, the increased burden of somatic mutations has led to the expression of numerous neoantigens, resulting in immunostimulation; patients with cancer having these features are expected to be optimal candidates for PD-1 blockade [787980]. Indeed, MSI has been used as a predictive biomarker for immune checkpoint inhibitors in colorectal cancer [81]. However, the efficacy of immunotherapy in MSI GC, which is known to show comparatively better prognosis and is usually observed as distal GC, has not been evaluated [82]. Four patients with MSI GC were enrolled in the KEYNOTE 012 study [75]. A phase II study of nivolumab with or without ipilimumab to evaluate its efficacy in MSI-high gastrointestinal tumors is ongoing [83]. Immunotherapeutic approaches in patients with MSI GC remain to be proven.
Gene expression studies in melanoma patients enrolled in the KEYNOTE 001 trial have identified a few gene signatures, including interferon-gamma 10-gene and expanded-immune 28-gene, as potential predictive markers of clinical response to pembrolizumab [84]. Interestingly, GC patients enrolled in the KEYNOTE 012 trial, harboring these gene signatures, showed improved survival [7585]. These findings are expected to encourage further studies with larger populations to identify these signatures as potential predictive biomarkers of response to immune checkpoint inhibitors.
Epstein-Barr virus (EBV) infection is known to increase the risk of GC by 10-fold, and EBV cancers account for approximately 10% of all GC cases [8687]. Interestingly, several studies have indicated that the PD-L1 gene is amplified more frequently in EBV-positive cancers than in EBV-negative cancers, suggesting that EBV GC is another possible target of immunotherapeutic agents [8889]. In addition, PD-L1-overexpressing EBV-positive GC shows upregulated interferon adaptive immune response [90], and is associated with an increased infiltration of immune cells into tumors [89]. Furthermore, tumor infiltration of immune cells was significantly associated with disease-free intervals in EBV GC, suggesting cellular immune response as a useful prognostic marker in this group [91]. In the KEYNOTE 012 trial, no EBV infection data were collected [75].
Approximately 50% of GC cases are thought originate due to Helicobacter pylori infection [92]. H. pylori infection triggers inflammation, resulting in altered gastric microenvironment, accelerated cancer cell transformation, and immune cell infiltration. In addition, H. pylori infection induces DNA methylation in tumor suppressor genes, and increases the levels of inflammation-related proteins, including tumor necrosis factor-alpha [93]. Many studies have reported T cell anergy during H. pylori infection [949596]. Furthermore, H. pylori infection upregulates PD-L1 expression in gastric epithelial cell lines [96]. Based on these findings, it might be hypothesized that H. pylori-related GC may respond well to immune checkpoint inhibitors, which remains to be proven.
In GC with chromosomal instability (CIN) and genomic stability (GS), there is no overexpression of PD-L1/2 or high loads of mutations, which suggests that these subgroups are less likely to be responsive to immunotherapy compared with other GC subtypes [80]. GCs are not associated with hyper-mutations but show aberrations in the CHD1, ARID1A, and RHOA genes, which are related to epithelial-mesenchymal transition. CIN GC usually occurs at the esophagogastric junction and has a tendency to harbor chromosomal deletions, alterations, and amplifications, resulting in abnormalities in genes, including EGFR, HER2, MET, RAS, BRAF, and VEGFR.
Future directions in immuno-oncology
Although trials on monotherapy with anti-CTLA-4 antibodies have been unsuccessful, PD-1/PD-L1 axis inhibitors have shown promising results in patients with GC. A phase III study of nivolumab versus placebo (ATTRACTION-2) showed favorable results. CTLA-4 and PD-1/PD-L1 axis interrupt lethal immune responses in cancer via reciprocal pathways [97], and several preclinical studies have shown possible synergistic effects of the combined checkpoint blockades [9899100]. Based on these findings, clinical trials on combination treatments containing nivolumab and ipilimumab have been conducted in malignant melanoma with favorable outcomes [101102103]. Therefore, several ongoing phase III studies evaluating the efficacies of PD-1/PD-L1 axis inhibitors and their combinations with anti-CTLA-4 inhibitors in GC patients are expected to yield significant findings with clinical implications.
In addition to the integration of immune checkpoint inhibitors, immunotherapy in combination with other target-specific agents could be considered. In a phase Ib study on renal cell carcinoma, pembrolizumab in combination with axitinib, an inhibitor of VEGFRs was found to be substantially effective [104]. Therefore, a phase III KEYNOTE 426 trial was started (NCT02853331). Accordingly, treatment with ramucirumab, a monoclonal antibody targeting VEGFR2, in conjunction with immune checkpoint inhibitors is a potential therapeutic strategy for GC. Recently, MEK inhibitors in conjunction with immune checkpoint inhibitors have been suggested to exert synergistic effects in microsatellite-stable (MSS) RAS mutant colorectal cancer; this combination is also a promising intervention in GC, which often involves the activation of the RAS-MEK-ERK pathway [105].
GC is a heterogeneous disease. Therefore, subpopulation studies investigating potential predictive markers, including EBV pattern, MSI status, and PD-L1 expression, are needed. However, diagnostic challenges for the evaluation of molecular mechanisms and difficulties associated with decreased sample size after filtering participants need to be addressed.
Cost-effective studies are crucial, given the lack of consensus regarding the ideal treatment duration and exorbitant costs of immunotherapeutic agents. To identify reliable therapeutic approaches, the identification of useful predictive biomarkers with credible diagnostic tools is crucial.
NEW DIRECTION OF CLINICAL TRIALS ON TARGET-SPECIFIC AGENTS
Considering that GC harbors a diverse range of genetic mutations and tend to carry high mutational loads [12106107], various target-specific agents may be investigated in GC treatment. However, as previously noted, only a few trials have been successful, resulting in the lack of new standard therapies [89]. The possible reasons underlying the failures are summarized below.
First, patient selection was not based on validated predictive biomarkers. Several failed studies, including EXPAND, REAL3, and GRANITE-1, did not involve the selection of participants who are expected to benefit from the experimental drugs [444565]. Compared with the ToGA trial [8] in which only patients with HER2 IHC3+ or FISH+ status were included, the TyTAN study [31] enrolled all patients with HER2 FISH+ status. As a result, 34% of the enrolled patients were expected to benefit less from HER2-targeting agents, according to the criteria used in the ToGA trial. Such inappropriately broad selections of patients were also performed in trials targeting c-MET, including the RILOMET-1 trial [61]. Although MET gene amplification by FISH was observed in about 10%–20% of GC cases [5859], MET protein overexpression was found in more than 50% of patients enrolled in the RILOMET-1 study [61], in which MET protein expression was analyzed by IHC staining. MET protein level analysis by IHC is reported to be unreliable for meaningful biomarker examination [108], and any trial in which more than 50% of all screened patients are registered, is challenging to conduct successfully.
The inappropriate combination of drugs may be another reason. The REAL3 trial used triplet chemotherapy combinations, which consisted of epirubicin, oxaliplatin, and capecitabine (EOC) as a backbone regimen [45]. Clinical outcome with the combination of EOC and panitumumab was poorer than that with EOC only (HR, 1.37; 95% CI, 1.07–0.76; P=0.013). Since epirubicin-containing triplet combinations are generally associated with highly toxic side effects, target-specific agents in combination with these regimens are ordinarily thought to be inappropriate. Combinations of 2 small-molecule inhibitors or a small-molecule inhibitor along with a cytotoxic agent are also generally avoided because maximum tolerated doses of these regimens could be too low (due to high toxicities) to achieve target inhibition.
Tumor heterogeneity is the most important factor underlying the failure of single-target agents. Even in the case of trastuzumab, the only proven HER2-targeting agent, the therapeutic efficacy is markedly diversified depending on HER2 heterogeneity, and this diverse pattern of HER2 expression is more prevalent in GC than in breast cancer [24]. HER2 IHC3+ samples also showed a heterogeneous pattern of staining in more than 30% of cases [109]. Considering focal distribution, target-specific inhibitors are expected to work only against selected tumors. The disappearance of HER2 expression is also regarded as a major cause of trial failure. HER2 expression disappeared in about 30% of patients who underwent first-line treatment [110]. The GATSBY trial, which explored potential second-line treatments in GC, involved the determination of the HER2 status of participants with tumor samples obtained prior to the first-line treatment [36]. The sequential loss of HER2 expression affected the study results. A similar case of failure was reported in the SHINE study, investigating the TKI targeting FGFR1–3 [66].
A recent report demonstrated that target genes in GC are diversely distributed by using a specially-generated tissue microarray with a multitude of tissue cores from the primary tumor and various metastases [111]. This study suggested that a single clinical cancer biopsy could limit treatment decisions, and multiple biopsies might be needed for deciding the most appropriate treatment plan. Furthermore, with rapid advances in next generation sequencing technologies, systematic analyses of therapeutic targets in GC are promising [112]. In terms of concerns about sequential alterations of gene targets, the real-time monitoring of primary tumor entities by analyzing circulating tumor cells from patient blood samples could be helpful [113].
CONCLUSIONS
Clinical outcomes in GC patients may be improved via appropriately designed clinical studies. Appropriate target selection and patient inclusion criteria are essential; however, tumor heterogeneity of GC remains an obstacle even with fine targets serving as driver mutations. Therefore, clinical trials investigating a single target are of little importance in predicting GC treatment outcome; accordingly, several studies have been unsuccessful over the past decade. A combination of several target-specific agents may be considered. However, the maximum tolerated doses of combinations determined by phase I study may not be adequate for target inhibition. Nevertheless, whether successful combinations of 2 or more target-specific agents can overcome this challenge is yet to be established.
In contrast to target-specific agents, immuno-oncologic agents are designed to regulate and boost anti-cancer immunity, without the need for targets and may overcome tumor heterogeneity. Among immuno-oncologic therapies, including cancer vaccines, oncolytic viruses, and chimeric antigen receptors, immune checkpoint inhibitors are the mainstay of clinical interventions in GC trials. MSI GC, bearing high loads of mutations, and EBV-related GC, overexpressing PD-L1, may be ideal candidates for immune checkpoint inhibitors. Based on other data, a checkpoint blockade is not excluded in patients even with MSS or PD-L1-negative GC. Recent data support that checkpoint inhibition in combination with MEK inhibitors may be associated with synergistic effects in RAS mutant MSS colorectal cancer [105]. In CIN GC carrying mutations of EGFR, HER2, or VEGFR, antibodies targeting HER2 or VEGFR2 in conjunction with immunotherapy are attractive therapeutic options.
Major challenges in GC management can be overcome via appropriate patient selection, the effective combination of drugs, and proper sequential treatment. Further efforts are imperative to explore and validate useful predictive biomarkers, which are crucial for patient selection. Preclinical studies exploring ideal combinations of drugs are also needed. Despite gaps in the currently available data, further studies in this direction may establish the new frontier in GC treatment.
 XML Download
XML Download