

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Behçet's disease (BD) is a multisystemic, chronic, relapsing systemic inflammatory disorder characterized mainly by oral and genital ulcers, uveitis, skin manifestations, and joint, vascular, CNS, and gastrointestinal involvements.123 When patients with BD present with predominant gastrointestinal symptoms and intestinal ulcerations observed objectively, they may be diagnosed with intestinal BD.45 The prevalence of intestinal BD is higher in East Asia, including Korea and Japan, than in Mediterranean countries.6 Similar to IBD, intestinal BD shows a fluctuating clinical course with repeated episodes of relapses and remissions.78 Gastrointestinal involvement of BD, often related to poor treatment responses and catastrophic bowel complications, can be life-threatening in some cases,910 although symptoms of intestinal BD range from mild abdominal discomfort to massive bleeding, fistula, or bowel perforation.67 Indeed, intestinal BD requires similar surgical interventions to those of CD, predicting a poor prognosis.11 However, clinical data regarding the diagnosis of intestinal BD and predicting factors for its disease activity and long-term outcomes are still limited because of its scarcity. The Korean IBD Study Group recently proposed novel diagnostic criteria and an index to assess the disease activity of intestinal BD. Here, we will review the progress in the diagnosis and assessment of the disease activity of intestinal BD.
DIAGNOSIS OF INTESTINAL BD
The incidence of gastrointestinal involvement in BD shows a remarkable geographic variation, ranging from 0% to 60%, which seems to be more prevalent in East Asia.612 Although the gastrointestinal involvement of BD may be related to a poor prognosis in affected patients, to date, no specific diagnostic criteria have been developed for intestinal BD because of its rareness and lack of clinical evidence.
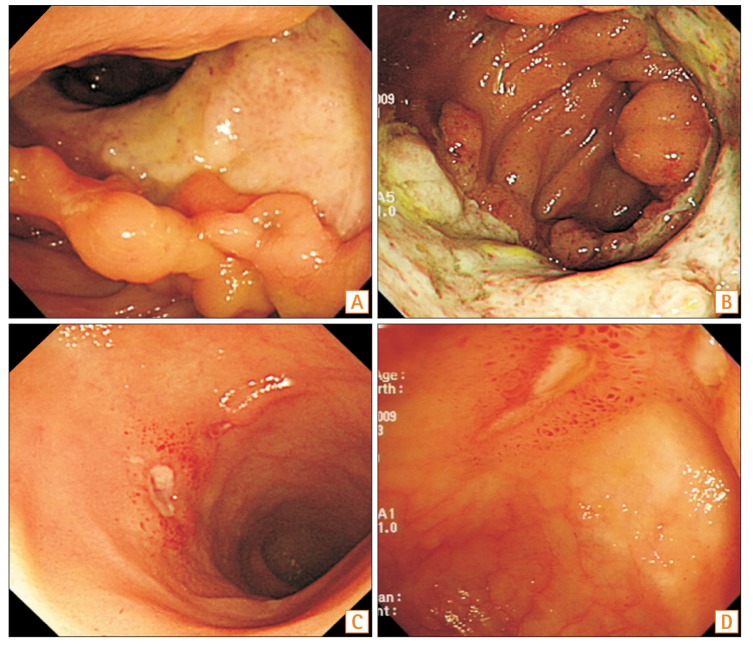
Intestinal BD is generally diagnosed if patients have both intestinal ulcerations and clinical findings of systemic BD. Diagnosis should be made considering the clinical, endoscopic, radiologic, and pathologic findings.1314 The clinical manifestations need to meet the diagnostic criteria of BD as suggested by the International Study Group for BD or the BD Research Committee of Japan.1516 The common gastrointestinal symptoms include abdominal pain, diarrhea, bleeding, and weight loss, and the typical intestinal ulcerations are defined as <5 ulcers that are oval in shape and deep with discrete borders located in the ileocecal area (Fig. 1).17 However, various ulcerations could be observed from aphthous ulcers to deep and penetrating volcano-shaped ulcers, and not only focal distribution but also diffuse ulcerations present in patients with intestinal BD.18 The representative pathologic findings of intestinal BD include the presence of vasculitis involving small- and medium-sized vessels and lymphocyte infiltration in the perivascular space.1920 The absence of a noncaseating granuloma would indicate intestinal BD rather than CD, although such a finding is identified in less than half of the CD cases.
1. Differential Diagnosis
Other diseases that mimic intestinal BD should be ruled out before intestinal BD is diagnosed, including tuberculosis, CD, nonspecific colitis, and drug-associated colitis.21 Intestinal BD and CD indeed share numerous similarities, such as nonspecific gastrointestinal symptoms, extraintestinal manifestations, wax-and-wane disease courses, and long-term clinical outcomes; thus, it is sometimes difficult to distinguish between the 2.711 However, clinically, oral and genital ulcerations are more common in intestinal BD, while perianal lesions, stricture, and fistula formations are more frequent in CD.1122 Endoscopically, longitudinal ulcers with a cobblestone appearance are frequently observed in CD, whereas intestinal lesions in intestinal BD tend to appear as few round-shaped, punched-out, deep ulcers with discrete margins, which are more prone to perforate.17 Lee et al.23 suggested simplified algorithms for the differential diagnosis of the 2 disease entities by investigating their colonoscopic features. Five colonoscopy findings, including a round ulcer shape, focal distribution, fewer than 6 ulcers, absence of aphthous lesions, and cobblestone appearance were independently dominant in intestinal BD, and by sequentially applying 2 variables with ulcer shape followed by distribution, the 2 diseases could be differentiated up to 92%.
Intestinal tuberculosis (ITB) may also be difficult to distinguish from intestinal BD and CD because of its overlap in endoscopic appearance and prevalent geographic regions. According to a study by Lee et al.,24 involvement of fewer than 4 segments, patulous ileocecal valves, transverse ulcers, and scars or pseudopolyps were observed commonly in ITB, and anorectal lesions, longitudinal ulcers, aphthous ulcers, and cobblestone appearance were seen frequently in CD. Using these colonoscopic parameters, ITB can be diagnosed correctly in 87.5% of the patients.
2. Novel Diagnostic Criteria for Intestinal BD
According to the Japanese consensus-based practice guidelines for the diagnosis of intestinal BD using a modified Delphi approach, patients should have both confirmed BD and intestinal lesions without other gastrointestinal diseases to enable a definite diagnosis of intestinal BD.21 Some patients with typical intestinal ulcers do not meet the diagnostic criteria of BD, and systemic manifestations may appear sequentially after several months or years after initial intestinal ulcerations in others.172526 One of the major concerns of the Japanese diagnostic criteria includes intestinal involvements in patients without clinical findings of BD. Lee et al.17 reported that the clinical and colonoscopic characteristics of patients with intestinal involvement who lack the systemic manifestations of BD were in accordance with the characteristics of those who fulfill the criteria. Shin et al.26 also showed that patients who have typical ulcerations without systemic BD symptoms tended to satisfy the BD criteria throughout the disease course. Another concern is that the characteristics of intestinal lesions are difficult to define. Simple intestinal ulcers are often considered as a variation of the same disease spectrum of intestinal BD because intestinal lesions initially presenting as simple ulcers could be eventually diagnosed as intestinal BD over time.2728 Therefore, to date, clinicians are apt to diagnose and manage intestinal BD even in patients who do not fully satisfy the systemic manifestation criteria for BD at the time of colonoscopy.
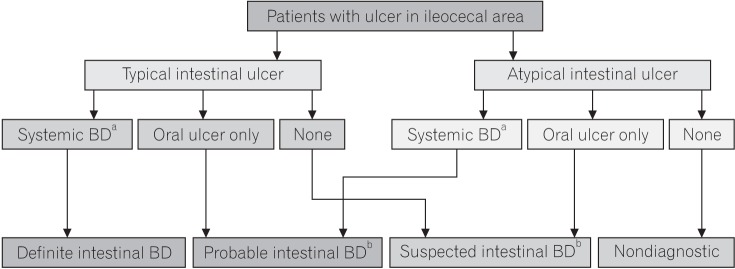
Owing to these unmet needs, the Korean IBD Study Group recently developed novel diagnostic criteria for intestinal BD.29 These diagnostic criteria were developed on the basis of the colonoscopic findings and extraintestinal systemic manifestations using a modified Delphi method. The extraintestinal manifestations were classified in accordance with the diagnostic criteria by the BD Research Committee of Japan16 that can reflect a temporal change better than the International Study Group for BD criteria during follow-up. The newly developed criteria categorized patients into 4 groups: definite, probable, suspected, and nondiagnostic (Fig. 2) and suggested a management strategy according to each category. Patients with typical intestinal ulcerations and extraintestinal symptoms who met the Japanese criteria were categorized as the “definite” intestinal BD group and managed for intestinal BD. Patients with typical intestinal ulcerations with only typical oral symptoms or atypical intestinal ulcerations and extraintestinal symptoms who met the Japanese criteria were categorized as the “probable” group. Patients with typical intestinal ulcerations without any extraintestinal symptoms or atypical intestinal ulcerations with only typical oral symptoms were categorized as the “suspected” group. Patients in the probable or suspected group needed to be followed up closely because a substantial number of patients are eventually diagnosed with intestinal BD. The “nondiagnostic” group included patients who had only atypical intestinal ulcerations without any extraintestinal manifestations. These newly developed algorithms for the diagnosis of intestinal BD might be useful, especially in patients with intestinal ulcerations in the ileocecal area who do not fully satisfy the diagnostic criteria of systemic BD.
DISEASE ACTIVITY MONITORING OF INTESTINAL BD
Intestinal BD showed a heterogeneous range of clinical courses over time. In a retrospective study by Jung et al.30 analyzing the clinical course of patients with intestinal BD who were regularly followed up for at least 5 years, majority of the patients (71.6%) had a mild clinical activity, whereas the remaining patients (28.4%) had multiple relapses or chronic symptoms. In addition, intestinal BD often requires surgery because of complications, including massive bleeding, fistula formation, and perforation.79 The cumulative rates of surgery were reported to be 31.6% at 5 years and 44.4% at 10 years after diagnosis, which were comparable to those of CD.11 Even after surgery, the cumulative clinical recurrence rates were shown to be 21.1% at 1 year and 51.1% at 5 years.11 Considering its unpredictable disease flare-ups and poor overall prognosis, the objective assessment of its disease activity is indispensable in determining the best therapeutic strategy and in assessing the treatment response.
1. Endoscopy
Endoscopy plays an essential role in the measurement of the disease extent and severity of IBD.31 Kim et al.18 analyzed the clinical outcomes of patients with intestinal BD according to the colonoscopy findings that volcano-type ulcerations were prone to show less favorable responses to medications, more frequent surgical intervention, and recurrence than the aphthous and geographic ulcerations. Lee et al.32 also suggested that more than 2 ulcers and volcano-shaped ulcers were associated with higher disease activities.
As mucosal healing has emerged as a treatment target in IBD, the need for endoscopy continues to increase.3334 In agreement with previous studies in IBD,3536 Yim et al.37 reported that mucosal healing was an independent factor for favorable clinical outcomes with a lower recurrence rate in patients with intestinal BD. The presence of active ulcerations was associated with a higher risk of disease relapse even in clinical remission status, which might implicate the role of mucosal healing as a therapeutic target in the management of intestinal BD.
In addition, endoscopy is considered the gold standard in the diagnosis of postoperative recurrence and prediction of clinical outcomes in IBD. The postoperative Crohn's endoscopic recurrence study revealed that early colonoscopy and step-up treatment are better than conventional drug therapy alone for the prevention of postoperative CD recurrence.38 Recently, our group developed an endoscopic scoring system predicting clinical relapse after surgery in patients with intestinal BD using colonoscopic findings, including ulcer size and numbers. Multiple and >20 mm-sized ulcers were related to clinical relapse after surgery in patients with intestinal BD (data unpublished). However, while widely accepted to represent the state of bowel inflammation, endoscopy still has limitations of cost, inconvenience, and invasiveness.
2. Biomarkers
To complement these drawbacks, various biomarkers have been studied to estimate the severity of inflammation and monitor the disease activities. Among laboratory markers, ESR and CRP are the most studied and considered the most representative.3940 ESR and CRP levels were well correlated with the disease activity of systemic BD,4142 and a higher CRP level was proven to be a predictor of relapse in patients with intestinal BD with 5-aminosalicylic acid/sulfasalazine treatment.43 In addition, cumulative recurrence rates and reoperation rates were higher in surgically treated patients with higher CRP levels than in those with lower CRP.44
Choi et al.45 found that the positive rate of anti-Saccharomyces cerevisiae antibodies was 44.3% in patients with intestinal BD; anti-S. cerevisiae antibody positivity was significantly associated with increased surgical rates. In addition, Shin et al.46 reported that the prevalence of anti-α-enolase antibody was 67.5% in patients with intestinal BD, and a cumulative steroid use was higher in patients with a positive anti-α-enolase antibody than in those with a negative antibody. Recently, serum soluble triggering receptor expressed on myeloid cells-1, which is known to play a role in the inflammatory response by stimulating the productions of proinflammatory cytokines,47 has been shown to increase in patients with intestinal BD; further, its levels showed a higher correlation with the disease activity of intestinal BD than CRP and ESR levels.48 In addition, a recent study found that levels of IL-12B involved in Th17 differentiation were significantly correlated with clinical and endoscopic activities of intestinal BD implicating its potential role as a biomarker.49 On the other hand, procalcitonin was able to differentiate infection from active inflammation in IBD in that it was not affected by the disease activity of intestinal BD but by a concomitant infection.50
Compared to serologic biomarkers, fecal biomarkers, such as calprotectin and lactoferrin, have the advantage in terms of increased specificity for intestinal inflammation.4051 Kim et al.52 suggested that similar to IBD, levels of fecal calprotectin were significantly higher in patients with typical ulcerations than in those with atypical ulcerations, and the absolute changes in fecal calprotectin and disease activity index for intestinal BD (DAIBD) showed a significant correlation during 3 months of treatment. However, to date, no single biomarker has been proven to be ideal in assessing the disease activity of intestinal IBD.
3. Disease Activity Index for Intestinal BD
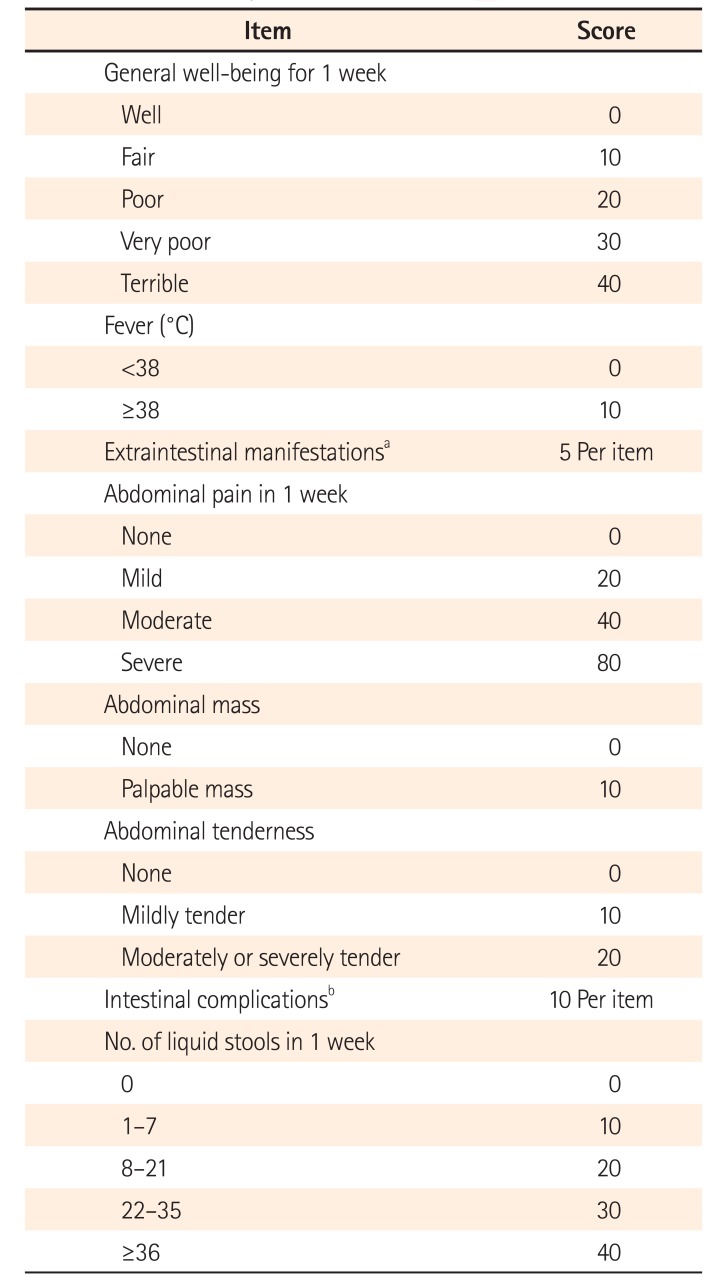
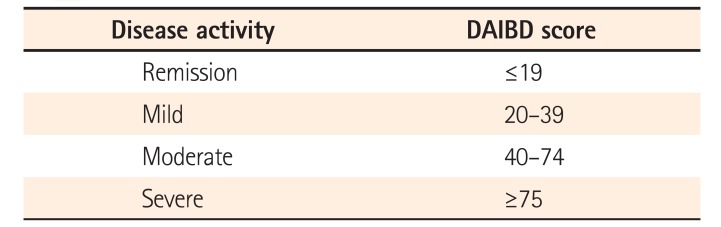
To date, there is no specific tool to assess the disease activity of intestinal BD; therefore, the measurement of its disease activity depends heavily on expert opinions or the use of other IBD indices, such as the CDAI.21 The Korean IBD Study Group accordingly developed a novel tool to measure the disease activity of intestinal BD.53 As a single clinical or laboratory parameter could not consistently reflect the level of intestinal inflammation, a multi-item measurement similar to CDAI54 and pediatric ulcerative colitis activity index55 was needed to evaluate the disease activity of intestinal BD. DAIBD consists of 8 items as follows: general well-being, fever, extraintestinal manifestations, abdominal pain, abdominal mass, abdominal tenderness, intestinal complication, and number of liquid stools (Table 1), ranging from a score of 0 to 325. Depending on the DAIBD score, the disease severity was divided into 4 groups (Table 2): quiescent (≤19), mild (20–39), moderate (40–74), and severe (≥75) diseases. DAIBD showed a better performance than CDAI in terms of good correlation with the physician's global assessment. DAIBD has also advantages over CDAI as it is a relatively simple 8-point index and is easily applied in the outpatient clinic. However, the recent study failed to show the correlation between DAIBD and endoscopic severity, similar to CD.3256 Meanwhile, a multinational web-based survey reported that even in Asian countries, physicians adopted different scoring systems to assess the disease activity of IBD.57 Further studies are mandatory to validate the usefulness of DAIBD in various populations and predict the clinical outcomes more precisely by considering both endoscopic factors and clinical activity indices.
CONCLUSIONS
Gastrointestinal involvement is one of the major causes of morbidity and mortality in BD. However, clinical data are limited because of the scarcity of intestinal BD cases, and to date, there has been no standardized diagnostic tool or pathognomonic finding for intestinal BD. Recently developed novel diagnostic criteria and a disease activity index might help physicians make a correct diagnosis and decide an appropriate treatment by assessing the disease activity of intestinal BD. Further international validation for these guidelines is needed, and biomarkers specific for intestinal BD in the diagnosis, disease activity assessment, and clinical outcome prediction should be investigated in the future.
 XML Download
XML Download