

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
A report from the Korea National Statistical office shows that cardiovascular disease (CVD) remains the leading killer, illustrating the continued burden of mortality arising from CVD. Mortality rate from CVD including cerebrovascular disease has been > 20% since 1983 and ranks next to cancer [1]. Thus, an effort has been made to identify potential mechanisms to explain the cardiovascular risks even in treated individuals.
In particular, one of the unfavorable features of CVD risk in Koreans is that hypertriglyceridemia concomitant with low high density lipoprotein (HDL)-cholesterol is very widely prevalent [2]. Additionally, the prevalence of metabolic syndrome (MetS) is high even in patients with a relatively lower body mass index (BMI) [3]. Finally, small dense low density lipoprotein (LDL) (sd-LDL) concentrations are higher in Koreans compared with those in Scots [4]. This raises the possibility that sd-LDL could be an independent risk factor for CVD through its metabolic associations with triglycerides (TG) and the presence of MetS particularly in Koreans whose LDL cholesterol levels are relatively lower than those of western societies [5].
The plasma lipoprotein profile accompanying a predominance of sd-LDL particles (phenotype B) is associated with an increased risk for CVD, as evidenced by case control studies of myocardial infarction [6-7] and angiographically documented coronary artery disease [8]. Some prospective studies also show the relationship between peak LDL particle size and CVD development [9-10].
Despite the high predominance of sd-LDL in Koreans, identifying factors responsible for high plasma levels of sd-LDL has not been studied. Therefore, this study investigated the factors that characterize the LDL phenotype and LDL particle size levels in healthy Korean women. We first compared features, including serum lipids, plasma LDL particle size, and dietary components between LDL phenotypes A and B to determine the factors influencing the levels of LDL particle size in healthy Korean women.
Subjects and Methods
Study subjects
Fifty-seven healthy women (mean age, 57.4 ± 13.1 yrs; range, 33-85 yrs) were included in the analysis. The subjects were all healthy non-smokers. Those who were taking hypolipidemic medications, hormone replacement therapy, or had been diagnosed with uncontrolled hypertension or type 2 diabetes mellitus were excluded. At the start of the study, we examined life style habits of each participant i.e., yes or no to regular exercise, cigarette smoking, alcohol consumption and dietary supplementation such as antioxidative vitamins and isoflavone, which could influence the variables studied. The purpose of this study was carefully explained to all participants, and their informed consent was obtained prior to participation. This study protocol was approved by the Institutional Review Board of Yonsei University College of Medicine and carried out in accordance with the Declaration of Helsinki.
Anthropometric parameters and blood collection
Body weight and height of the subjects were measured, and body mass index (BMI) was calculated. Venous blood samples were collected from the forearm into EDTA-treated (plasma for LDL particle size) and plain (serum for other lipid profiles and fasting glucose) tubes after fasting. The tubes were immediately covered with aluminum foil and placed on ice until they arrived at the analytical laboratory. The blood samples were centrifuged to yield plasma or serum, and stored at -70℃ until analysis.
Dietary survey
We acquired dietary data using a semi-quantitative food frequency questionnaire (SFFQ), as described by Suh et al. [11] and Nam et al. [12]. Briefly, the SFFQ contains 87 food items generally consumed daily by Koreans. Several food categories were included, for example, rices and their products (i.e., white rice, whole grains cooked or uncooked formed), noodles such as cold noodles, hot noodles, instant noodles, and ramen, bread and pains, cereals and their products, potatoes and starches, simple sugars, vegetables, and fruits. Each subject was asked to report their usual frequency of consumption and their usual portion size during the past year. During the interview, food models and reference utensils were shown to subjects to help them estimate portion size. The frequency of consumption was measured on a nine-point scale: never, 1 time/month, 2 times/month, 1 time/wk, 3 times/wk, 5 times/wk, 1 time/day, 2 times/day, and 3 times/day. The questionnaire was used for mixed dish recipes. Intake was assessed on four scales: one-half, one, one and a half, and a double portion size. Nutrient intake was calculated using Korean food composition tables and other published data [13-14].
Serum lipid profiles and glucose concentrations
Serum cholesterol, LDL-cholesterol, and HDL-cholesterol were measured with commercially available enzymatic kits (Choongwae, Seoul, Korea). Serum triglyceride levels were analyzed using a total glycerol test kit (Roche, Basel, Switzerland). All measurements were conducted on a Hitachi 747 auto-analyzer (Hitachi Ltd. Tokyo, Japan). Apolipoproteins AI (apoAI) and B (apoB) were measured by immunoturbidometric assay (Express 550 Plus analyzer). Total apolipoprotein CIII (apoCIII), one of the major apolipoproteins found in TG-rich particles, was measured in triplicate by sandwich assay (International Immunology Corp., Murrieta, CA, USA). Fasting serum glucose concentrations were measured using the glucose oxidase method with a Beckman Glucose Analyzer (Beckman Instruments, Irvine, CA, USA).
Plasma LDL particle size and determining LDL phenotype
Non-denaturing polyacrylamide gradient gel electrophoresis with lipid staining of the plasma was performed to determine peak LDL particle diameter, as described previously [15]. Briefly, electrophoresis was performed on whole plasma and on the plasma fraction with density < 1.063 kg/L (prepared by ultracentrifugation) using Pharmacia PAA 2/16% gradient gels (Uppsala, Sweden). Stained gels were scanned with a Transidyne RFT scanning densitometer (Ann Arbor, MI, USA), and peak particle diameters of the major LDL subclasses were calculated from calibration curves using standards of known size. A smaller LDL peak diameter indicated a relative abundance of sd-LDL particles. Subjects were grouped on the basis of two modes; one grouping comprised subjects with buoyant-mode profiles (peak LDL particle diameter ≥ 256 Å including large LDL subclass pattern: ≥ 264 Å, and intermediate LDL subclass pattern: 256 Å ≤ peak LDL particle diameter ≤ 263 Å) designated phenotype A, and the other subjects with dense-mode profiles (peak LDL particle diameter ≤ 255 Å), were designated phenotype B [16].
Statistical analysis
The SPSS 12.0 software package was used for statistical analysis (SPSS, Inc. Chicago, IL, USA). We used Pearson's correlation coefficient to evaluate the relationships among variables and stepwise multiple regression analyses to identify factors influencing LDL particle size levels. Data are presented as means ± standard deviations. Each variable was examined for normality, and abnormally distributed variables were log-transformed. Differences in the values between phenotypes A and B were evaluated using Student's t-test or the Mann-Whitney U-test (nonparametric t-test). P-values < 0.05 were considered statistically significant.
Results
Comparisons of baseline characteristics between phenotypes A and B
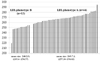
Baseline characteristics of the 57 healthy, non-smoking women are shown in Table 1. Subjects were grouped as LDL phenotype A (mean size, 269.7 Å; range, 257.34-294.63, n = 44) or LDL phenotype B (mean size, 248.2 Å; range, 219.4-254.57, n = 13) (Fig. 1.). As shown in Table 1, age and the proportions of subjects who exercised, consumed alcohol, and were postmenopausal were similar between the two groups. Mean BMIs were significantly higher in the subjects with LDL phenotype B than those with LDL phenotype A. As expected, the subjects with phenotype B showed significantly higher levels of serum TG (P < 0.001), total cholesterol (P < 0.001), LDL-cholesterol (P < 0.05), apoB (P < 0.001), and apoCIII (P < 0.005) but significantly lower levels of HDL-cholesterol (P < 0.001). The concentrations of apoAI and fasting glucose were not different between the two groups.
Comparisons of energy and nutrient intakes between phenotypes A and B
Table 2 shows the estimated energy and nutrient intakes between the two groups. The percentage of carbohydrates as total energy intake [carbohydrate (% En)] was significantly higher in subjects with LDL phenotype B than those with LDL phenotype A (P < 0.05), whereas the percentage of fat for total energy intake [fat (% En)] was significantly lower in the subjects with LDL phenotype B than those with LDL phenotype A (P < 0.05). Retinol intake was greater in the subjects with LDL phenotype B than those with LDL phenotype A (P < 0.01). No significant differences were observed in other nutrient intakes between the two groups.
Associations between LDL particle size and selected macronutrient intake and biochemical measurements
We evaluated the associations between the levels of LDL particle size with selected biochemical measurements (TG, total cholesterol, LDL cholesterol, HDL cholesterol, and apo AI, B, and CIII) and macronutrient intake [% En, percent of energy intake from carbohydrate, fat and protein], which were significantly different between the two groups (Table 3). The results showed that LDL particle size levels were negatively correlated with TG, total cholesterol, apoB, and apoCIII. The LDL particle size levels were positively correlated with HDL cholesterol and apoAI. As LDL particle size was highly associated with TG, the parameters were adjusted for TG. When adjusted for plasma TG, the significant correlations between LDL particle size and total cholesterol, LDL cholesterol, and apoAI, B, and CIII disappeared. A weak relationship was observed between LDL particle size and HDL cholesterol after adjusting for TG (P = 0.058). LDL particle levels were negatively associated with carbohydrate (%) intake (P < 0.005) and positively associated with fat (%) intake (P < 0.005). These correlations remained significant after adjusting for TG (P < 0.05 for both). Additionally, we identified factors influencing LDL particle size levels using a stepwise multiple regression analysis. Baseline characteristics (i.e., age, BMI, menopause, exercise, alcohol consumption), lipid profiles (i.e., TG, HDL-cholesterol and apolipoproteins) and macronutrient intake [carbohydrate (%) and fat (%)] were used as independent variables in the model. Among the input variables, we included lipid profiles and macronutrient intake, which were significantly different between the LDL phenotype groups and also significantly correlated with LDL particle size after adjusting for TG. This model revealed that serum levels of TG (P < 0.001) and carbohydrate (%) intake (P < 0.05) were closely associated with LDL particle size levels (Table 4).
Discussion
The aim of this study was to investigate the major factors that characterize the LDL phenotypes and the levels of LDL particle size, a potential risk factor for CVD and related diseases, in healthy Korean women. The present results confirmed that LDL particle size (LDL phenotype) was closely correlated with circulating TG levels and demonstrated, for the first time, that LDL particle size was significantly associated with dietary carbohydrate intake in Korean women.
Many studies have reported that sd-LDL, LDL III, or the LDL phenotype B are associated with elevated circulating TG levels, abdominal adiposity, increased concentrations of apolipoprotein B, and decreased concentrations of HDL-cholesterol [7,8,17]. In addition, sd-LDL has been postulated to be a major risk factor for CVD [7]. According to a report by Austin et al. [6], subjects with a LDL profile dominated by sd-LDL have a three-fold increased CVD risk. Griffin et al. [8] also reported a seven-fold increase in CVD risk for sd-LDL concentrations > 100 mg/dl. Several physiological mechanisms have been attributed to the greater atherogenicity of dense than buoyant LDL [18-20]. sd-LDLs are taken up less readily by LDL receptors, penetrate more readily into arterial tissue, bind more tightly to arterial proteoglycans, and are oxidized more rapidly than larger LDL particles [18-20].
sd-LDL prevalence in Asian Indians is significantly higher than that in Caucasians [21]. Cho et al. [4] also reported that both male and female Koreans have higher relative proportions of LDL III compared to those in Scots. The elevated level of sd-LDL might be due to differences in genetics or environmental factors such as dietary habits among ethnic groups. Additionally, several studies have confirmed that the predominance of sd-LDL is also significantly influenced by specific genes related to lipid metabolism, including the cholesteryl ester transfer protein, the LDL receptor, manganese superoxide dismutase, lipoprotein lipase, APOE, and APOA5 [22] In the present study, the regression analysis revealed that serum levels of TG and dietary carbohydrate intake were independent factors for LDL particle size, which is supported by previous reports [21,22]. It is well known that circulating TG is strongly associated with LDL particle size and density [22]. There is also evidence that LDL III concentration increases linearly through the whole range of circulating TG concentration in Korean men, whereas in Scottish men, there was a threshold of 108 mg/dl triglyceride above which there was a positive association [4], suggesting that circulating TG may interact with certain dietary patterns (i.e., high or low carbohydrate intake) and/or with genetic backgrounds (Asians or Caucasians) to form sd-LDLs. LDL particle size was also correlated with circulating levels of HDL-cholesterol, apoB, apoAI, and apoCIII. However, these associations were no longer significant after adjusting for serum TG levels, suggesting that they were mediated through metabolic associations with high levels of circulating TG. In contrast, numerous studies have investigated the association between dietary macronutrient proportions and lipid profiles, particularly the effects of alterations in dietary carbohydrate on fasting blood TG concentrations in postmenopausal women [23-25]. The increased carbohydrate intake observed in this study may cause the synthesis of free fatty acids in the liver, which, in turn, could potentially stimulate the production of large TG-rich very low density lipoprotein, a precursor of sd-LDL particles [26]. Despite rapid transitions in dietary patterns over time in Korea [27], dietary carbohydrates are still the major source of energy intake in Korea. Thus, it is possible that high carbohydrate intake is somehow related to the expression of these phenotypes through its metabolic associations.
We focused on female subjects in this study because dyslipidemia characterized by lower HDL cholesterol, smaller LDL cholesterol particle size, and higher TG is a strong contributing factor to the increased CVD risk, which is more remarkable in females than males [28]. The influence of MetS on the increased risk for CVD is greater among women than among men [29,30]. Particularly, pregnancy, lactation, gestational diabetes mellitus, preeclampsia, polycystic ovary syndrome, hormonal contraceptives, and menopause are considered factors influencing MetS and CVD risk together with central adiposity, dyslipidemia, hypertension, and hyperglycemia in women [31]. In addition, a study conducted in Koreans [32] reported that abdominal obesity is significantly related to carbohydrate intake in women but not in men. Furthermore, the Korean National Health and Nutrition Examination Survey reported that subjects with MetS consume a higher percentage of energy from carbohydrates than those without MetS, which was remarkable in women [33]. Therefore, special dietary efforts emphasizing the limitation of high carbohydrate intake for Korean women would improve the increasing burden of CVD risk. Krauss [22,34] showed a strong linear relationship between decreased fat/increased carbohydrate intake and the prevalence of the LDL subclass pattern B in healthy men, indicating that the prevalence of pattern B in men consuming 30% fat is ~30-35%, which corresponds to the consumption of > 55% carbohydrate [22,34]. Taken together, the cut-off point for carbohydrate intake in Koreans to maintain a healthy LDL phenotype needs to be established, as Koreans consume a relatively higher percentage of energy from carbohydrates compared to that of Western people, although the effect of ethnicity still must be considered.
This study had several limitations. It was a cross-sectional study and had a small sample size. Additionally, information such as glycemic index needs to be included to address the associations more precisely. Nevertheless, the present study was meaningful because it was conducted in a very homogenous group of Koreans. In summary, the present study showed that LDL particle size (LDL phenotype) was closely correlated with circulating TG levels and demonstrated, for the first time, that particle size is significantly associated with dietary carbohydrate intake in Korean women.




 XML Download
XML Download