

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ascorbate (vitamin C) is a fundamental vitamin for human life as an important antioxidant by blocking damage from free radicals,1 and acts as a cofactor for hydroxyl enzymes in collagen synthesis which has been thought to prevent tumor spreading.23 On the other hand, high-dose vitamin C can act as a prooxidant, conferring selective toxic effects on cancer cells.4 Also, it may exert anti-inflammatory activity resulting in suppression of tumor proliferation, angiogenesis, and metastasis.5 High-dose vitamin C supplementation has been widely used as complementary and alternative medicine, particularly in cancer patients.6 Although there is a paucity of clinical research data to confirm the effects of vitamin C on cancer, some interesting case reports have suggested the clinical prospect of high-dose vitamin C therapy.78 One of these is similar to our report, except it involved multiple pulmonary metastases originating from renal cell cancer.8 Here, we report a case of regression of multiple pulmonary metastases originating from hepatocellular carcinoma after high-dose vitamin C therapy.
CASE REPORT
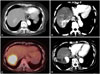
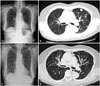
A 74-year-old woman was found to have a 2.2-cm liver mass with multiple satellite nodules (T2N0M0) on abdominal-pelvic CT (APCT) in January 2011 (Fig. 1A). Protein induced by vitamin K absence or antagonist-II (PIVKA II) was within normal range, 28 mAU/mL, but alpha fetoprotein (AFP), 4040.05 ng/mL, was high, and anti-hepatitis C virus was positive. The patient initially received transarterial chemoembolization (TACE) in February 2011, but locally recurrent hepatocellular carcinoma with multiple pulmonary and mediastinal lymph node metastases were found on positron emission tomography-computed tomography (PET-CT) scan in July 2011 (Fig. 2A and B) and APCT in September 2011 (Fig. 1B). She refused further treatment, including sorafenib tosylate (Nexavar, Bayer Health-Care AG, Leverkusen, Germany), and then visited our clinic with anorexia and general weakness in September 2011 requesting high-dose vitamin C to manage her symptoms. Twenty grams of vitamin C in 250 mL normal saline was initially administered via an ante-cubital vein twice a week in September 2011 after urine analysis and renal function were confirmed to be within normal range. To neutralize acidic pH (3.5-5.0) of vitamin C, it was mixed with NaHCO3, resulting in pH 6.2 (UniC®, 500 mg/mL from Unimed Pharmaceuticals, Seoul, Korea). In addition, normal saline was changed to distilled water as vitamin C dose increased to avoid too much intake of volume and sodium and too high concentration. Furthermore, magnesium sulfate 1 g was blended in the fluid to prevent vascular irritation.9 Notably, she did not have glucose-6-phosphate dehydrogenase deficiency. Prior to April 2012, no significant progression or regression of her multiple pulmonary metastases was found on serial chest X-ray, although she reported improved general wellbeing. In July 2012, multiple pulmonary nodules were found to have completely regressed on chest X-ray (Fig. 2C), which was confirmed on PET-CT scan in September 2012 (Fig. 2D). However, a 5.5-cm hepatic mass still remained on abdomen ultrasound and PET-CT scan (Fig. 1C). Considering her good performance status, we recommended repeated TACE, but she declined. Therefore, high-dose vitamin C administration was continued for more than a year. In July 2013, she finally decided to undergo TACE in addition to the high-dose vitamin C treatment. Subsequently, three rounds of TACE were performed. After the fourth round of TACE, the hepatic mass was found to have entirely regressed (Fig. 1D), and both PIVKA II and AFP levels had returned to normal range. The serial changes in AFP and PIVKA II levels are shown in Table 1. The patient denied any use of other anti-cancer medications or alternative therapies except pain medication for her intermittent abdominal pain. She was quite tolerant of high-dose vitamin C during the entire treatment period, but thirst was an occasional complaint, which was easily remedied by water intake.
DISCUSSION
In the 1970s, Cameron and Pauling reported that high-dose vitamin C had therapeutic effects in cancer.10 Early clinical studies showed that high-dose vitamin C administration conferred survival benefit compared to control groups.1112 However, a subsequent clinical study at Mayo Clinic failed to show significant differences in survival between an oral vitamin C administration group and the control group.13 In addition to these studies in which oral vitamin C was tested, a recent pharmacokinetic study suggests that high concentrations of intravenous vitamin C are toxic to cancer cells.14 Hoffer, et al.15 reported that when 1.5 g/kg of vitamin C was administered, plasma concentrations over 10 mM could be maintained for 4.5 hours. Some authors suggest that the oral administration of vitamin C at the Mayo Clinic could have failed to achieve effective plasma concentrations, and that effective concentrations can only be reached by intravenous administration.16 Therefore, further clinical studies to evaluate the anti-cancer effects of intravenous high-dose vitamin C are warranted.
Potential mechanisms of action of vitamin C on cancer cells remains uncertain, but recent experimental data suggest some possible mechanisms. First, vitamin C has a pro-oxidant effect at higher concentrations. Chen, et al.17 reported that high-dose vitamin C generated hydrogen peroxide (H2O2) in the extracellular fluid, which then entered into cells. H2O2 is able to accelerate the production of additional reactive oxygen species (ROS) such as aldehydes. These ROS are capable of several effects, including DNA damage, cell membrane dysfunction, and cellular adenosine triphosphate depletion in cancer cells due to reduced levels of antioxidant enzymes such as glutathione peroxidase, superoxide dismutase, and catalase. These processes are not found in normal cells and may lead to death of cancer cells.1819 Second, vitamin C may modulate inflammation resulting in increase of host resistance to cancer. Cho, et al.20 demonstrated that highly concentrated vitamin C decreased the production of interleukin-18, which is related to tumor cell growth, proliferation, and migration. Chen, et al.21 reported that the expression of hypoxia-inducible factor-1α protein, which is associated with tumor growth, is inhibited by vitamin C in an animal study. In addition, Mikirova, et al.22 demonstrated that C-reactive protein level which is correlated with disease activity was reduced after high-dose vitamin C treatment in cancer patients.
In conclusion, we describe a case of regression of multiple pulmonary metastases after treatment with high-dose vitamin C, which enabled a subsequent trial of TACE, eventually leading to complete remission of the primary hepatocellular carcinoma. Notably, intravenous vitamin C administration has an advantage in terms of safety compared to other conventional cancer therapies. Our patient did not show any complications or serious side effects, except for mild thirst. Although there is controversy over the effect of vitamin C on cancer, intravenous administration of high-dose vitamin C could be attempted in patients who refuse conventional therapy. Also, we hope to find a common denominator in accumulated case reports that might offer clues to which cases vitamin C administration could be an effective cancer therapy.

 XML Download
XML Download