

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The most common morphology observed in the human spine is 24 presacral mobile vertebra, including seven cervical, 12 thoracic, and five lumbar vertebra. Although the number of cervical vertebra is fixed at seven, the number of thoracic and lumbar vertebra can vary (1234567).
Correct numbering of the vertebra is critical for avoiding operative errors. However, accurate enumeration can be challenging due to spinal variants, including anomalies in the total number or distribution of vertebra, transitional vertebra (e.g., thoracolumbar transitional vertebra [TLTV] and lumbosacral transitional vertebra [LSTV]), and other anomalies (689101112). A high percentage of errors occur in patients with spinal variants (2131415). Although correct numbering of the LSTV has been documented in previous literature (691112), less information is available regarding the numbering of other spinal variants (61617).
Therefore, the purpose of this study was to compare spinal enumeration methods used to establish the first lumbar vertebra in patients with spinal variants.
MATERIALS AND METHODS
Patients
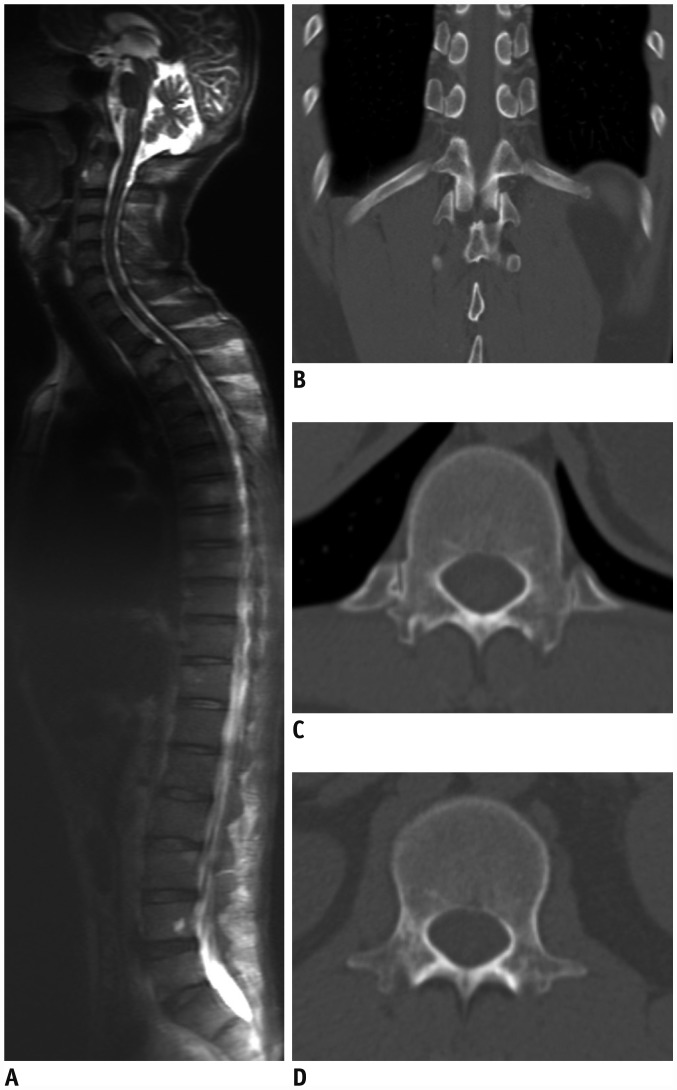
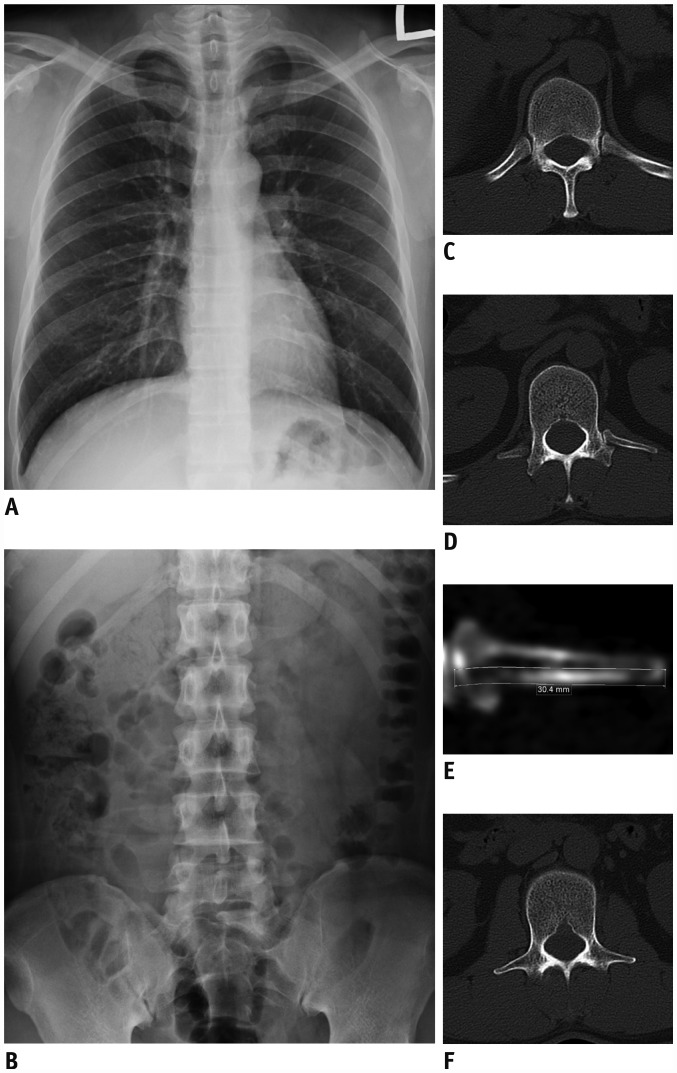
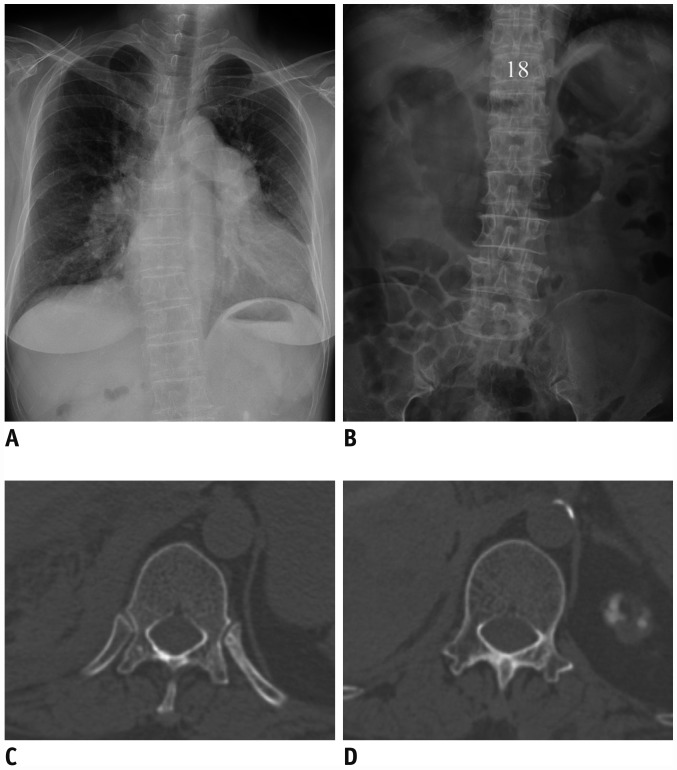
Our Institutional Review Board approved this study, and the requirement for informed consent was waived. This study was a retrospective review of 1446 consecutive patients who underwent CT of the spine, including the thoracolumbar and lumbosacral junctions, for back pain between March 2012 and July 2016. We excluded 1346 patients who did not have spinal variants (n = 1269) or additional images (n = 77) (i.e., whole-spine radiographs, magnetic resonance [MR] imaging scans or computed tomography [CT] imaging scans) that would allow us to count the number of presacral mobile vertebra (Fig. 1A). Posteroanterior chest and supine abdominal radiographs were regarded as wholespine radiographs because these images could be used to count the number of presacral mobile vertebra (Fig. 2A, B). Although it was not possible to count down from the first cervical vertebra, the number of cervical vertebra is known to be fixed at seven (1234567). Therefore, on the posteroanterior chest and supine abdominal radiographs, the number of presacral mobile vertebra could be determined by counting down from the first rib-bearing thoracic vertebra and adding the seven cervical vertebra. In addition, posteroanterior chest radiographs included the cervicothoracic junctions. Thus, the first rib could be differentiated from a cervical rib because the former arises from a superiorly directed transverse process, while the latter articulates from an inferiorly directed transverse process (18). For the same reason, chest CT and abdominal CT images were also regarded as whole-spine CT scans. The existence of spinal variants in each case was evaluated by a radiologist, based on axial spine CT with curved planar reformatting (CPR) images and images to determine the number of presacral mobile vertebra (i.e., both posteroanterior chest and supine abdominal radiographs, both chest CT and abdominal CT images, whole-spine radiographs, MR imaging, or CT imaging). Spinal variants included the following: 1) alteration of the typical distribution of 12 thoracic and five lumbar vertebra (Fig. 3), 2) anomalous total number of presacral mobile vertebra (e.g., 22, 23, or 25) (Fig. 1), and 3) TLTV or LSTV (Fig. 2). Park et al. (19) suggested differentiating vertebral segments at the thoracolumbar junction as TLTV or non-TLTV (thoracic or lumbar) segments on the basis of definitive criteria for differentiating most caudal ribs in consideration of several variants of the thoracolumbar junction. In accordance with the previous literature (1319), a thoracic vertebra is defined by the presence of paired ribs that are 3.8 cm or greater in length and originate from the facet at the pedicle (or the body) of the vertebra (Figs. 1B, C, 2C, 3C). A lumbar vertebra was identified as a vertebra without articulating ribs, without facets for ribs on the pedicle (or the body of the vertebra), and with fused transverse processes (Figs. 1D, 2F, 3D) (13). TLTV were defined as any segments that did not meet the criteria for thoracic or lumbar vertebra in the thoracolumbar junction (Fig. 2D) (19). CPR images were used for the accurate measurement of rib length. Rib length was measured by drawing a line at the midpoint of the rib width from the proximal head of a rib to the distal body (Fig. 2E) (19). Only type I or II LSTV, as defined by the Castellvi classification (20), were included in this study, because we focused our analysis on the number of presacral mobile vertebra. Finally, 100 consecutive patients with spinal variants were included in the study.
Spinal CT
All CT images were acquired with a dual-source CT scanner (Somatom Definition Flash; Siemens Healthcare, Erlangen, Germany). Patients were scanned with a detector configuration of 128 × 0.6 mm with combined modulation (CARE Dose 4D; Siemens). Standard-of-care spinal CT imaging was performed at 275 quality reference mAs. All CT imaging was performed using the following parameters: pitch, 0.7; gantry rotation time, 0.5 seconds; section width, 1 mm; and reconstruction increment, 0.7 mm.
Image Analysis
Establishment of the First Lumbar Vertebra in Spinal Variants: Morphologic Analysis of the Thoracolumbar Junction
Wigh and Anthony (21) stated that the true nature of lower vertebral segmentation can only be established with images that include the thoracolumbar junction, thereby allowing correct identification of the first lumbar vertebra. Park et al. (19) also suggested that morphologic analysis of the thoracolumbar junction may improve the accuracy of spinal enumeration. Therefore, in this study, establishment of the first lumbar vertebra through morphologic analysis was performed on images that included the thoracolumbar junction.
On the basis of the morphologic analysis of the thoracolumbar junction performed by Park et al. (19), two radiologists (readers 1 and 2) independently assessed vertebral segment types at the thoracolumbar junction, then classified them as the thoracic vertebra, lumbar vertebra, or TLTV. As described above, a lumbar vertebra was defined as a vertebra without articulating ribs, without facets for ribs on the pedicle (or the body of the vertebra), and with fused transverse processes (Figs. 1D, 2F, 3D) (13). On the basis of this definition, the first lumbar vertebra was established on axial CT images. Then, to differentiate thoracic vertebra from TLTV, the two radiologists used axial CT scans with CPR images.
During morphologic analysis of the thoracolumbar junction, each reader was blinded to the whole-spine images that allowed the number of vertebra to be counted and to the other reader's results. After the first lumbar vertebra was established, each reader labeled the first lumbar vertebra by counting in a cranial-to-caudal manner (e.g., 19th, 20th, or 21st segment), using images to determine the number of presacral mobile vertebra (i.e., both posteroanterior chest and supine abdominal radiographs, both chest CT and abdominal CT images, whole-spine radiographs, MR imaging, or CT imaging) (Figs. 1D, 2F, 3D). Inter-observer agreement between the two readers in establishing the first lumbar vertebra through morphologic analysis of the thoracolumbar junction was analyzed with kappa statistics. Kappa values were categorized as slight (0–0.20), fair (0.21–0.40), moderate (0.41–0.60), substantial (0.61–0.80), or nearly perfect (0.81–1.00) agreement (22).
Comparison of Spinal Enumeration Methods for Spinal Variants
In the traditional method of spinal numbering (4910112324), the first lumbar vertebra is determined by counting down from the second cervical vertebra or the first thoracic vertebra, under the assumption that there are 12 thoracic vertebra. In the above method, the 20th vertebra is always the first lumbar vertebra. Accordingly, herein, the first lumbar vertebra identified by the above enumeration method was compared with that identified through morphologic analysis of the thoracolumbar junction. First, reader 1 detected the 20th vertebra by counting in a cranial-to-caudal manner (Figs. 1A, 2A, B). The 20th vertebra was then categorized through morphologic analysis of the thoracolumbar junction by reader 1 as thoracic, lumbar, or TLTV (Figs. 1B, C, 2D).
RESULTS
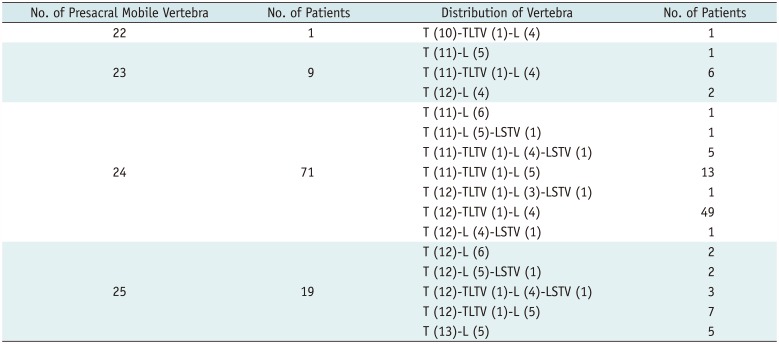
One hundred patients (62 men and 38 women) with spinal variants were included in this analysis. Mean age of the patients was 47.9 years (range, 19–88 years). Twenty-nine patients (29.0%) had an anomalous number of presacral mobile vertebra: there were 22 presacral mobile vertebra in one patient; 23 in nine patients; and 25 in 19 patients. All patients showed anomalous distribution of vertebra. TLTV were observed in 85 patients (85.0%) and LSTV were observed in 13 (13.0%). Nine patients (9%) had both TLTV and LSTV (Table 1). A comparison of the methods used for the correct identification of the first lumbar vertebra in spinal variants is presented in Table 2.
Establishment of the First Lumbar Vertebra, according to Morphologic Analysis of the Thoracolumbar Junction
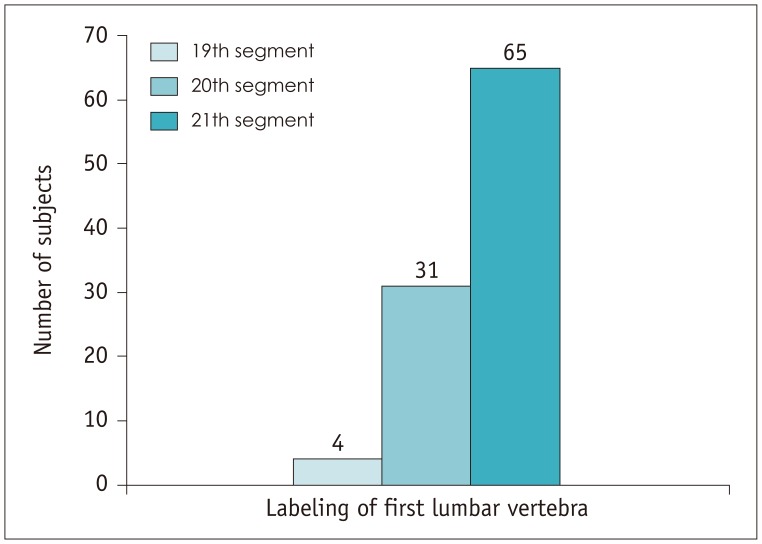
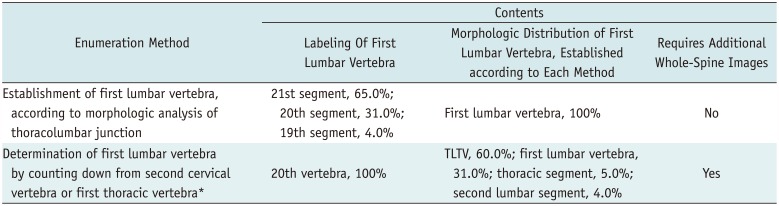
The first lumbar vertebra, as established through morphologic analysis of the thoracolumbar junction, was labeled by each reader as the 21st segment in 65.0% of the patients, as the 20th segment in 31.0% of the patients, and as the 19th segment in 4.0% of the patients (Fig. 4). Inter-observer agreement between the two readers in determining the first lumbar vertebra on the basis of morphologic analysis was nearly perfect (κ value: 1.00). Although there was a discrepancy in the distribution of vertebra in one case, it did not affect establishment of the first lumbar vertebra. In that case, 11 thoracic vertebra, one TLTV, and five lumbar vertebra were identified by reader 1, while 12 thoracic vertebra and five lumbar vertebra were identified by reader 2. This disagreement in values was because of a discrepancy in the measurement of the rib length by the two readers. Reader 1 considered the 19th vertebra as a TLTV, because the vertebra had paired separated bones, one of which was less than 3.8 cm in length, although it articulated with the facet at the pedicle. In contrast, reader 2 considered the 19th vertebra as a thoracic vertebra, because reader 2 regarded the paired ribs as being 3.8 cm or greater in length.
Determination of the First Lumbar Vertebra by Counting Down from the Second Cervical Vertebra or the First Thoracic Vertebra
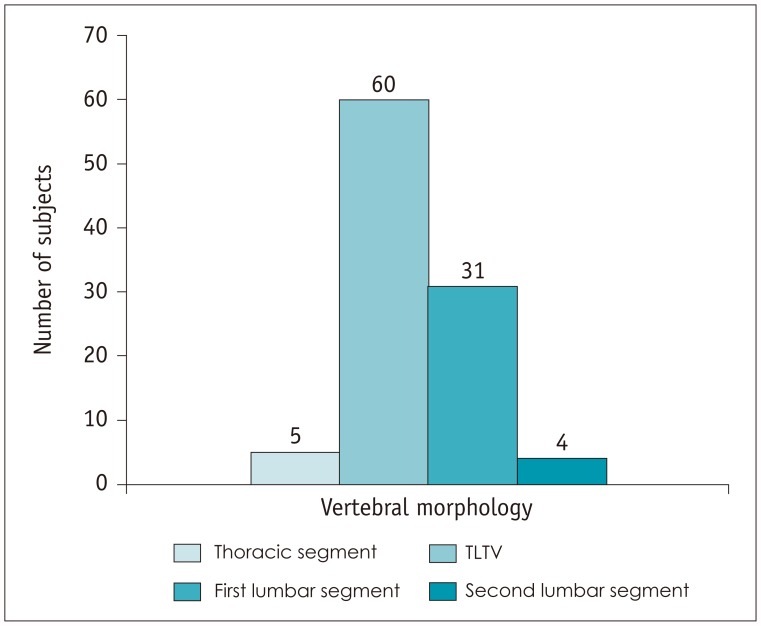
The 20th vertebra, which was identified by counting in a cranial-to-caudal manner by reader 1, was morphologically classified as a TLTV in 60.0% of the patients, as the first lumbar segment in 31.0% of the patients, as the second lumbar segment in 4.0% of the patients, and as a thoracic segment in 5.0% of the patients (Fig. 5).
DISCUSSION
We compared the spinal enumeration methods used to establish the first lumbar vertebra for patients with spinal variants. On the basis of morphologic analysis of the thoracolumbar junction, establishment of the first lumbar vertebra was consistent with the literal meaning of “the first lumbar vertebra.”
In most previous studies, the establishment of lumbar segments in patients with LSTV has been performed with the assumption that there are seven cervical and 12 thoracic segments (91011161723). However, Carrino et al. (6) suggested that LSTV are associated with anomalies in the total number of presacral segments. Therefore, it may be inappropriate to assume that there are seven cervical and 12 thoracic segments when numbering the lumbar vertebra in patients with certain spinal variants, including LSTV. Notably, in this study, the 20th vertebra exhibited the morphologic traits of the first lumbar vertebra in just 31.0% of the patients with spinal variants. Thus far, no reports have numerically presented the aforementioned results.
As mentioned above, Wigh and Anthony (21) stated that the true nature of lower vertebral segmentation can only be established with images that include the thoracolumbar junction, thereby allowing correct identification of the first lumbar vertebra. According to Hughes and Saifuddin (12), LSTV levels can be confirmed after the first lumbar vertebra has been correctly established. Although several studies (91112) have evaluated vertebral numbering in LSTV, studies using images that include the thoracolumbar junction have not been conducted previously. Although Carrino et al. (6) labeled the first lumbar vertebra as the first non-rib-bearing vertebra on lumbar MR imaging, they did not consider thoracolumbar junction variants. Accordingly, in this study, the first lumbar vertebra was established through morphologic analysis of the thoracolumbar junction through consideration of several variants of the thoracolumbar junction, with the method used by Park et al. (19). Thus, identification of the first lumbar vertebra by morphologic analysis of the thoracolumbar junction should be used as the reference standard to determine vertebral segments. The next step is to apply this method to the numbering of LSTV and to the evaluation of anatomic markers (e.g., aortic bifurcation, right renal artery, conus medullaris, iliolumbar ligament, and iliac crest), which are used as landmarks for the localization of lumbar vertebral segments.
In this study, inter-observer agreement in determining the first lumbar vertebra, based on morphologic analysis of the thoracolumbar junction was nearly perfect (κ value: 1.00). Given the definition of a lumbar vertebra (identified as a vertebra without articulating ribs, without facets for ribs on the pedicle [or the body of the vertebra], and with fused transverse processes) (13), the establishment of the first lumbar vertebra showed high reliability. Identification of the first lumbar vertebra on the basis of morphologic analysis can be performed on any axial images that include the thoracolumbar junction, without the need for images that cover the complete spinal axis.
In this study, the total number of presacral mobile vertebra varied from 22 to 25. It is known that 23 and 25 presacral mobile vertebra are commonly observed in cases of spinal variants, while cases of the number of presacral mobile vertebra varying between 22 to 26 have been reported (25).
Lumbosacral transitional vertebra were observed in a relatively small percentage of the patients (13.0%) in our study, while TLTV were more common (89.1%). The only types of LSTV included in this study were type I or II LSTV, based on the Castellvi classification (20), because we focused on analyzing the number of presacral mobile vertebra. Therefore, the prevalence of LSTV was lower than that of TLTV.
This study had several limitations. First, relatively few patients with spinal variants were evaluated. Future studies with larger sample sizes are necessary. Second, the comparison between methods in this study was not conducted in clinical practice. Therefore, future multidisciplinary studies are necessary.
In conclusion, the establishment of the first lumbar vertebra on the basis of morphologic characteristics of the thoracolumbar junction in patients with spinal variants, which was consistent with the morphologic traits of vertebral segmentation, was achieved with nearly perfect inter-observer agreement.
 XML Download
XML Download