

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dynamic contrast-enhanced (DCE)-magnetic resonance imaging (MRI) is a quantitative functional MRI technique that provides information about tumor vascularity and perfusion, which can be used as pharmacodynamic and surrogate outcome biomarkers in cancer patients who are being treated with anti-vascular agents (1).
The vast majority of DCE-MRI in oncologic clinical trials and practice is aimed at assessing tumors in the torso. With DCE-MRI, patients are scanned continuously for several minutes while being allowed to breathe shallowly (1). However, the image quality of free-breathing DCE-MRI of the torso is greatly impaired by respiratory motion artifacts when using conventional three-dimensional (3D) gradient-echo (GRE) T1-weighted imaging (T1-WI) sequences, such as volumetric interpolated breath hold examination (VIBE) (2).
To overcome these respiratory motion artifacts, motion-resistant image acquisition schemes have been developed including radial 3D GRE T1-WI acquisition, radial-VIBE, and controlled aliasing in parallel imaging results in higher acceleration-VIBE (CAIPIRINHA-VIBE) (2345). When radial VIBE is combined with k-space-weighted image contrast reconstruction (KWIC)–known as radial VIBE with KWIC view-sharing and hereinafter referred to as radial-VIBE–it can generate time-resolved sub-frame images that enable DCE-MRI with high temporal resolution. Radial acquisition schemes are less motion-sensitive than conventional VIBE (c-VIBE), enabling free-breathing MRI examinations (2). CAIPIRINHA-VIBE uses a modified parallel acquisition technique (PAT), which lessens respiratory motion artifacts in particular by reducing scan time (678).
However, to our knowledge, no study has evaluated the effects of breathing motion on the DCE-MRI images acquired from these sequences. Therefore, we aimed at conducting a phantom study using a respiratory-motion-simulating platform to compare motion effects on DCE-MRI images among CAIPIRINHA-VIBE, radial-VIBE, and c-VIBE sequences. We assessed the effects of free breathing in terms of the efficacy of motion correction, motion-related artifacts, signal stability, and signal-to-noise ratio (SNR).
MATERIALS AND METHODS
We did not require approval from any kind of Ethical Committee because this was a phantom study. Two authors who are employees of Siemens Healthcare provided technical advice for MRI acquisition but did not participate in the data analysis or interpretation.
Phantom Construction
We modified a standardized quantitative imaging biomarkers alliance (QIBA) DCE-MRI phantom version 2 (9); the detailed information of this phantom is described in a prior study (3). Briefly, this phantom is composed of two rings of tubes containing 50 mL of NiCl2 solutions with different concentrations.
Moving Platform Construction
To simulate the breathing movement, we built a moving platform that consisted of a phantom holder with wheels, a plastic cover box, a handle, and a rail (Fig. 1). During MRI scanning, the DCE-MRI phantom was placed on the phantom holder with wheels, which was movable along the rail, which simulates the movement of internal organs according to respiratory motion; the handle was connected to the moving phantom holder. We cut shallow furrows in the handle at every 1 cm so that the researcher could consistently move the platform at a constant speed of 1 cm/sec. The plastic cover box was fixed, and the MR body coil was placed on top of the cover box.
MRI Acquisition
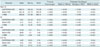
Using a 3T MR scanner (MAGNETOM Skyra; Siemens Healthcare, Erlangen, Germany) with standard body and spine coil arrays, we acquired the MRIs using CAIPIRINHA-VIBE, a prototypical radial-VIBE, and c-VIBE sequences in both moving and static modes. We obtained repeated series of each sequence over six minutes with a temporal resolution of five seconds, for a total of 72 time points. If we had shortened the temporal resolution of the DCE-MRI, we could have obtained more time points, but we suspected that temporal resolution of 5 seconds could be sufficient to reflect the first pass after the contrast agent injection and to meet the QIBA recommendation (9). The detailed MRI parameters are summarized in Table 1.
For the CAIPIRINHA-VIBE sequence, we used an acceleration factor of four (two in the phase-encoding direction and two in the partition-encoding direction) with a reordering delta shift of 1. Radial-VIBE uses a “stack-of-stars” trajectory, i.e., k-space data are acquired using radial sampling in the in-plane directions and Cartesian phase encoding along the through-plane direction (101112). During the radial-VIBE image acquisition, the full-frame data were obtained over 30.6 seconds with a view-interleaved radial acquisition scheme, specifically angle-bisection reordering, and KWIC reconstruction (13) was applied in order to generate six time-resolved, sub-frame images of 5.1-seconds temporal resolution; we used the time-resolved sub-frame images only for the radial-VIBE image analysis.
We scanned the phantom in a moving mode to simulate breathing motion using CAIPIRINHA-VIBE, radial-VIBE, and c-VIBE. Specifically, a well-trained researcher went into the MR examination room and manually moved the handle that was connected with the phantom holder; to minimize variability due to manual motion, an alarm clock was set to beep every second. The researcher repeatedly moved the platform, superiorly for 3 seconds and inferiorly for 3 seconds at a rate of 1 cm/sec to simulate breathing motion with a respiratory cycle of 6 seconds. Thereafter, the phantom was scanned statically using CAIPIRINHA-VIBE, radial-VIBE, and c-VIBE in order to obtain standard references to compare with images in a moving mode.
Image Analysis
Image Data Sets
From the DCE-MRI images obtained in a moving mode, we generated motion-corrected images using a dedicated software (Tissue 4D; Siemens Healthcare, Erlangen, Germany). We conducted motion correction with a non-rigid registration technique that aligned the dynamic data set to a defined reference volume by transforming each individual pixel so that the image pixels were displayed in the same geometrical position for both data sets. The advantage of the non-rigid registration is that local changes caused by for example, breathing, can be mapped correctly without having to correct organ or bone positions that are not affected by the local motion (14). Consequently, we could acquire three image sets (i.e., static images, moving images, and motion-corrected images) of each sequence (CAIPIRINHA-VIBE, Radial-VIBE, and c-VIBE) and use them for data analysis.
The Effects of Breathing Motion on the DCE-MRI Images
We visually assessed the effects of breathing motion on the three image sets (static, moving, and motion-corrected) of each sequence (CAIPIRINHA-VIBE, radial-VIBE, and c-VIBE). In particular, we evaluated the motions and shapes of the tubes in the phantom, as well as motion-related artifacts, and compared them between the three image sets.
Signal Stability
To evaluate how much the signal intensity of a subject varied over a DCE-MRI acquisition time (i.e., six minutes), we placed a circular region of interest (ROI) in the tube with the most concentrated NiCl2 solution for each image set of the three sequences and recorded the signal intensities of the ROIs at 72 time points over 6 minutes. We then plotted the measured signal intensities over time (hereafter referred to as time-intensity plots). For the quantitative assessment of the signal stability, we calculated the means and standard deviations (SDs) of the signal intensity from the 72 time points in each sequence. We then derived the coefficients of variation (CoVs) of the signal intensity by dividing the SDs by the means. The CoV (%) is a standardized measure of the dispersion of a distribution, and a small CoV indicates better signal stability (15).
Signal-to-Noise Ratio
We calculated SNR using a method based on a single image voxel (161718). In MRI images acquired using radial-VIBE or parallel imaging, such as CAIPIRINHA-VIBE, in which noise distribution can be inhomogeneous, SNR based on a single image voxel is known to be more accurate than conventional SNR based on two separate image voxels, i.e., one in the tissue and one in the background to measure the signal intensity and the noise, respectively. In this method based on a single image voxel, SNR is derived from the ratio of the mean and the SD of the signal intensity in repeated “identical acquisitions” over time (16). According to this method, the ROI was drawn at the tube that held the NiCl2 solution with the highest concentration along 72 sequential time points of MR images to measure the means and SDs of single image voxels for each time point.
Statistical Analysis
We compared the signal intensity, SD, and SNR according to motion mode within a sequence using a one-way repeated-measure ANOVA with a post hoc t test with Bonferroni correction. We compared the CoVs (%) according to motion mode within a sequence using Levene's test. We performed all statistical analyses using SPSS version 21.0 (IBM Corp., Armonk, NY, USA). p values less than 0.05 were considered statistically significant.
RESULTS
The Effects of Breathing Motion on DCE-MRI Images
Videos of the dynamic scanning using CAIPIRINHA-VIBE, radial-VIBE, and c-VIBE in static, moving, and motion-corrected moving modes are presented in the supplementary material. We believe these Supplementary Movie 1 (in the online-only Data Supplement) to be the most important data to obtain an overall intuitive sense of all image sets for the three sequences.
Figure 2 displays the captured images of dynamic scanning using CAIPIRINHA-VIBE, radial-VIBE, and c-VIBE in static, moving, and motion-corrected moving modes, which were aligned according to time (Fig. 2). Static images acquired using all three sequences showed a stable location of the phantom without substantial artifacts. Moving images and motion-corrected images showed the unique characteristics of each sequence.
For the CAIPIRINHA-VIBE, images of moving mode without motion correction demonstrated the up-and-down movement of the phantom; notably, the shape of the tubes was maintained during the up-and-down movement, although the overall shape of each tube was mildly distorted. After motion correction, the vertical motion of the phantom was resolved as if motion correction works as rigid registration. In addition, the tubes maintained their shapes without significant distortion. For the radial-VIBE, neither moving nor motion-corrected images displayed significant motion of the phantom, indicating the motion-insensitivity of this sequence. However, the round shape of each tube was degraded due to streak artifacts derived from the radial acquisition scheme, and these streak artifacts did not improve after motion correction. Regarding the c-VIBE, the moving images without motion correction showed phantom motion with significant related blurring, which substantially disrupted the original round shape of the tubes. Motion correction could not adjust for the vertical motion or the related blurring of the phantom.
Signal Stability
The time-intensity plots of the three image sets we obtained from the three sequences and CoVs (%) of the signal intensities are presented in Figure 3. The means and SDs of the signal intensities of all image sets are presented in Table 2. Static image sets of all three sequences showed stable signal intensity over 6 minutes (Fig. 3, blue lines), with a very low CoV (0.09% in CAIPIRINHA-VIBE, 0.03% in radial-VIBE, and 0.21% in c-VIBE). These CoVs were close to 0, indicating that the variation in MRI signal intensities for the static mode was negligible in all sequences. In contrast, moving and motion-corrected image sets showed unique patterns of signal intensity plots according to the characteristics of each sequence.
For CAIPIRINHA-VIBE, time-intensity plots demonstrated that moving images showed fluctuating signal intensities according to the vertical motion of the phantom (Fig. 3A, green line). Notably, after motion-correction, the variation in signal intensities decreased dramatically (Fig. 3A, red line). The CoV also decreased markedly from the moving (18.65) to the motion-corrected (2.56) image set. Indeed, the mean signal intensity and CoV of the motion-corrected images did not differ significantly from those of the static images (p > 0.05). These findings suggest that motion correction for aligning the subjects worked very well for CAIPIRINHA-VIBE by enhancing its motion insensitivity.
In radial-VIBE, the fluctuation of signal intensities on the time-intensity plots was similar in both non-motion-corrected and motion-corrected images; the mean signal intensities between the non-motion-corrected and motion-corrected images did not differ significantly (p = 0.074), which reflects that there was no significant motion in the phantom images due to the motion insensitivity of radial-VIBE. The CoV after motion correction (15.84) even increased, -compared to the images in moving mode (8.90), due to the non-rigid registration of streak artifacts (p < 0.001). These findings indicate that variations in signal intensity in non-motion-corrected and motion-corrected images mainly derived from motion-related streak artifacts rather than the movement of the subjects.
Regarding c-VIBE, the fluctuation of signal intensities on time-intensity plots was similar in both moving and motion-corrected images. There were no significant differences in the mean signal intensities (p > 0.999) or the CoVs (p = 0.153) of the moving and motion-corrected images. These findings indicate that motion correction may not be helpful for improving the image quality of c-VIBE moving images.
Signal-to-Noise Ratio
The SNR according to motion mode within each sequence differed significantly by sequence (p < 0.001) (Table 2). Both CAIPIRINHA-VIBE (3.37 for the moving state and 9.41 for the motion-corrected state; p < 0.001) and radial-VIBE (4.3 for the moving state and 4.96 for the motion-corrected state; p < 0.001) had improved SNRs after motion correction. In c-VIBE, the SNR worsened with motion correction, which indicates that the overlapped motion-corrected images of the distorted phantom negatively affected the SNR.
DISCUSSION
In our phantom study, in terms of breathing motion artifacts and signal stability, the use of CAIPIRINHA-VIBE with motion correction might have been better than radial-VIBE and c-VIBE for free-breathing DCE-MRI. CAIPIRINHA, a recently developed PAT scheme, modifies the acquisition pattern by shifting the sampling positions (i.e., delta shift) from their normal positions in the partition-encoding direction. By using the extra delta shift, CAIPIRINHA can compensate for the inherent aliasing artifact caused by applying high acceleration factors (19).
We postulate that the motion-resistant characteristics of CAIPIRINHA-VIBE mainly rely on reducing the image distortion during motion due to its advanced PAT scheme in both the partition-encoding and frequency-encoding directions (678). The shape of the phantom tubes was maintained without after-images motion, so that motion correction could align the images of moving subjects as seen on the supplemental material and Figure 2A. In addition, the measured signal intensities of the moving subject in the motion-corrected images were similar to those of the static subject (Fig. 3A) and showed excellent stability (CoV, 2.56%) over 6 minutes. These characteristics enabled us to reliably use the measured signal intensities for pharmacokinetic analysis to calculate perfusion parameters.
MRI images using CAIPIRINHA-VIBE for the moving mode showed mildly distorted images due to PAT and in-folding artifacts. PAT artifacts are known to be related to higher in-plane spatial resolution and a higher acceleration factor. In a previous study, the PAT artifact did not significantly hamper the overall image quality of gadoxetic-acid-enhanced liver MRI (19). The ghosting of edges is also closely related to the order of the k-space sampling.
It is worth comparing the characteristics of CAIPIRINHA-VIBE with those of radial-VIBE and c-VIBE, which are both commonly used for DCE-MRI in the torso. Notably, on the moving mode acquired with radial-VIBE, there was no motion of the phantom in the images (Fig. 2B). These results support that radial-VIBE is motion-insensitive due to its radial k-space sampling scheme to acquire data in a spoke-wheel fashion (212). However, radial-VIBE images were noisy and substantially degraded in the moving mode due to the streak artifacts that are characteristic of radial-VIBE due to under-sampling and/or susceptibility-related effects (122021). Indeed, the SNR of radial-VIBE was inferior to that of CAIPIRINHA-VIBE (4.96 vs. 9.41 for motion-corrected images), and the signal stability of radial-VIBE in the moving state was also not good (CoVs, 8.9% with moving images and 15.84% with motion-corrected images).
In radial-VIBE with KWIC view-sharing, with the long temporal footprint, the acquisition time for a fully sampled image (i.e., full-frame image) might have been another source of image degradation in the moving mode (2, 22). With KWIC, the peripheral k-space of a sub-frame image shares data from neighboring subsets obtained at different time points, whereas the central k-space of each sub-frame image uses data acquired from a single timely subset (221). Although KWIC was developed to increase the image quality of sub-frame images, unfortunately, breathing motion effects accumulated during the time to acquire a full-frame image may negatively influence the sub-frame images. In our study, we acquired a full-frame image for 30.6 seconds and generated six sub-frame images. Therefore, each sub-frame image could be influenced by breathing motion over 30.6 seconds rather than its frame time of 5.1 seconds. In contrast, CAIPIRINHA-VIBE and c-VIBE did not have this issue and were exposed to the breathing motion only for the acquisition time.
In terms of c-VIBE, it was originally developed to acquire 3D T1-weighted volumetric-interpolated images during a single breath-hold (723). c-VIBE has been known to be sensitive to motion artifacts because it uses rectilinear Cartesian k-space sampling. Our phantom study also demonstrated that c-VIBE was substantially degraded with both moving and motion-corrected images due to image blurring, distortion and after-images. In addition, the measured signal intensities in c-VIBE may not be reliable because overlapped after-images of the moving subject may mask the true variation in signal intensity along time points. Therefore, it may not be appropriate to use c-VIBE for free-breathing DCE-MRI.
Motion correction function is generally incorporated into commercial software used for analyzing DCE-MRI. However, motion correction is mainly used to align dynamic images to a reference image. In our study, we demonstrated that motion correction works efficiently when the objects move with preserved original shape, such as for CAIPIRINHA-VIBE. However, motion correction may not improve the distortion of subject images or artifacts, as demonstrated in the c-VIBE and radial-VIBE phantom images.
This study has a few limitations. The phantom used in this study obviously cannot completely represent the human body, and unexpected effects may have influenced MRI image quality. Similarly, the moving phantom platform is not identical to natural respiration movement in humans. For example, the liver does not move vertically in a straight line during true respiration (24); instead, liver movement is more complex, with cranio-caudal, lateral, and anterior-posterior motions (2526). In spite of these limitations, however, our study clearly visualized motion effects on each sequence and provided quantitative indices such as signal intensity, SD, SNR, and CoV during simulated breathing motions. Therefore, this preliminary phantom study may serve as a baseline study in establishing free-breathing DCE-MRI protocols.
In conclusion, our phantom study suggests that CAIPIRINHA-VIBE might be the best sequence for free-breathing DCE-MRI after motion correction, and it provides excellent image quality. Additional clinical studies should be undertaken to apply this result to real practice.




 XML Download
XML Download