

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Isolated acute nontraumatic cortical subarachnoid hemorrhages (cSAHs), also called convexal subarachnoid hemorrhages and convexity subarachnoid hemorrhages, are rare cases of bleeding in the subarachnoid space. They are localized to the convexities of the brain, usually several cortical sulci, without involving the brain parenchyma or extending into the interhemispheric fissures, basal cisterns, or ventricles. Unlike conventional subarachnoid hemorrhages (SAHs), rupture of the intracranial arterial aneurysm may not induce a cSAH. Various etiologies are described, such as cerebral venous thrombosis, posterior reversible leukoencephalopathy syndrome (PRES), reversible cerebral vasoconstriction syndrome (RCVS), coagulopathy, vasculitidis, vascular malformations such as pial arteriovenous malformations, dural arteriovenous fistulas, cavernomas, cerebral amyloid angiopathy (CAA), brain abscesses, atherosclerotic carotid disease, and primary and secondary brain neoplasms (1234567891011121314). Kumar et al. (1) suggested two main etiologic groups including cSAH patients < 60 years old presenting with thunderclap headaches that are ascribed to RCVS; and, cSAH patients > 60 years old presenting with transient focal symptoms and frequently exhibiting features suggestive of CAA under imaging methods (114). However, the ischemic stroke, especially the cerebral infarction or vasculopathy of extra- and intracranial arteries, such as high-grade stenosis, is not considered a common etiology of cSAHs.
We analyzed the associated radiologic findings of magnetic resonance imaging (MRI) of the brains of cSAH patients at a single center, in order to emphasize the importance of ischemic strokes as a common cause of cSAH.
MATERIALS AND METHODS
Study Plan and Patient Group
Our hospital's Institutional Review Board approved this retrospective study.
Patient Exclusion Criteria
We reviewed medical records, including hospital notes, laboratory data, and imaging studies, to exclude traumatic SAH and patients who exhibited the spreading of blood into Sylvian or interhemispheric fissures, as well as those with basal cisterns. We also excluded patients with intracerebral bleeding that may have ruptured into the subarachnoid space, patients with damage to the brain parenchyma adjacent to the cSAH, and patients with a large degree of cerebral infarction adjacent to the cSAH. Patients with only superficial siderosis were also excluded from the study. Moreover, patients with preceding episodes of head trauma, intracranial aneurysms, or thrombolytic therapy were excluded.
We retrospectively searched the radiologic reports of all the patients identified with cSAHs by initial brain CT scans or MRI at a single institution. From August 2005 to February 2014, fifteen cSAH patients were admitted to our institution including seven males and eight females with an average age of 47 years (range: 30 to 79 years). The patients who exhibited cSAH in the initial brain CT imaging underwent brain MRI for the further evaluation of combined pathologies. Thus, all patients with cSAH underwent brain MRI and magnetic resonance angiography (MRA). A retrospective analysis was conducted on the patients' medical history, clinical presentations, and brain MRI findings. Three (20%) patients had diabetes mellitus (DM), three (20%) patients had hypertension (HTN), and one (7%) had both. One (7%) patient had atrial fibrillation. One (7%) had chronic kidney disease and double primary cancers of the lung and prostate. One (7%) had previous myocardial infarction (Table 1). All the patients had a normal platelet count, prothrombin time, and activated partial thromboplastin time.
MR Imaging Protocol
Brain MRI and MRA systems operating at 1.5T (Signa Excite; GE Healthcare, Milwaukee, WI, USA) and 3.0T (Discovery MR 750; GE Healthcare) were available. The brain MRI included an axial fluid-attenuated inversion recovery (FLAIR) image, a diffusion- weighted image (DWI), a contrast-enhanced T1-weighted image (T1WI), and a gradient echo (GRE) T2*-weighted sequence. The MRA was performed using the time-of-flight method.
The contrast-enhanced T1WI was obtained by intravenous injection of 20 cc Meglumine Gadoterate (Dotarem; Guerbet, Paris, France) at 3 mL/s in each patient.
A brain dynamic susceptibility contrast perfusion study using MRI was performed in eleven cases. Perfusion maps showing the cerebral blood volume, cerebral blood flow, mean transit time, and time to peak were obtained by post-processing.
RESULTS
Among the fifteen cases involving cSAHs, eight (53%) involved cSAHs above the frontal cortex, and three (20%) involved cSAHs along the central sulcus. Three other cases (20%) exhibited cSAHs in the parietal area, and in one case (7%), bleeding occurred in the temporal area. All cSAHs were observed in the FLAIR images. The GRE images also adequately represented cSAHs.
The patients experienced a variety of symptoms. Primary motor or sensory change was regarded as the most common symptom. Nine (60%) patients exhibited hemiplegia, involuntary movement, or transient sensory loss. The latter involved the loss of consciousness, which occurred in two (13%) patients. Two (13%) patients complained of headache, and one (7%) reported dizziness.
Regarding the combined pathologies of the cSAH, eleven (73%) patients exhibited acute cerebral infarctions in the ipsilateral hemisphere on the DWIs. Four of the eleven patients had an acute cerebral infarction without extra- or intracranial vasculopathy. Vasculopathy of the intracranial arteries was observed in five of the eleven patients with cerebral infarction; of the five patients, three had stenosis of the intracranial arteries, and one had the occlusion of the right middle cerebral artery (MCA) M1 portion, and one had a dissection of the left anterior cerebral artery A2 portion. The remaining two patients with acute cerebral infarction had the stenosis of the extracranial arteries.
Two (13%) patients exhibited stenosis of the intracranial artery that supplied blood flow to the vascular territory containing the cSAH, without evidence of cerebral infarction. Both had the stenosis of the left MCA.
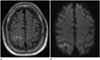
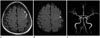
Figs. 1 to 4 showed cases of typical cSAH associated with an ischemic stroke, such as acute cerebral infarction and the highgrade stenosis of extra- or intracranial arteries.
Only one (7%) patient showed multiple intracerebral hemorrhage (ICH), which satisfied the Boston criteria for probable CAA (16). The remaining patient (7%) did not have any combined radiological abnormalities and exhibited only a cSAH. Table 2 presented the concise results.
Eleven patients who underwent brain dynamic susceptibility contrast perfusion study employing MRI showed no perfusion defect; however, three of the eleven patients exhibited the hyperperfusion state of the infarcted area. This could be considered a "luxury perfusion" after the acute cerebral infarction.
DISCUSSION
cSAH is rarely considered as a type of nonaneurysmal subarachnoid bleeding due to its varied etiologies. The etiologies of cSAH are under ongoing debate. Kumar et al. (1) suggested that RCVS and the CAA could be the major etiologies of cSAH. Beitzke et al. (15) also reported that RCVS is a major etiology of the cSAH in patients ≤ 60 years old, but RCVS could not be confirmed in these patients via angiograms. The exact pathophysiologic mechanism of cSAHs in patients with RCVS is unclear; however, there is speculation that it arises from abrupt changes in the cerebral arterial tone (1718). Patients > 60 years have an increased association of cSAHs with the CAA (15). Spitzer et al. (19) and Refai et al. (20) reported that PRES is the major underlying etiology of cSAH.
In contrast to these previous reports, our study showed that the ischemic stroke is the major etiology of the cSAH. Ischemic stroke, including cerebral infarctions, extra- or intracranial arterial stenosis, and intracranial arterial dissections was the confirmed cause in thirteen of fifteen cases (87%). Among the combined ischemic stroke disease entities, cerebral infarction was the most common in the cSAH patients. Some cases with cerebral infarction involved a combination of underlying stenosis and the dissection of the intracranial arteries.
Three letters to the editor reported cases similar to those considered in our study. Geraldes et al. (21) reported two cases of cSAH associated with acute carotid artery occlusion on the unilateral side; Kleinig et al. (22) described three cases of cSAH with bilateral internal carotid artery (ICA) stenosis; and Chandra et al. (23) also described a cSAH case with severe ICA stenosis. These authors could not explain the underlying mechanism but proposed that the acute alteration of the hemodynamic stress may damage the already maximally dilated pial collateral vasculature, leading to cSAHs. They proposed that systemic disturbances such as a sudden rise in blood pressure or a coagulation disorder in the presence of pre-damaged vessels account for these coincidental observations (212223). Some of our cases, particularly those of intracranial arterial stenosis without cerebral infarction, supported this hypothesis.
A possible underlying mechanism of cSAHs is as follows. Changes in the blood-brain barrier (BBB) reportedly occur in an acute or chronic ischemic insult (24252627282930). BBB abnormalities are reported in patients with small-vessel diseases secondary to HTN and DM (28). Particularly for lacunar strokes, BBB dysfunction was confirmed as a part of the pathogenesis (29). The disruption of the BBB during ischemia, hypoxia, or a hemorrhage progresses by two steps. The initial opening of the BBB is reversible and associated with the activation of matrix metalloproteinases. The second opening of the BBB occurs 24 to 48 h after a reperfusion, depending on the length of the ischemia. The BBB is damaged after these two steps, and its permeability increases (28). The qualitative visualization of Gadolinium-diethylenetriaminepenta- acetic acid (Gd-DTPA) indirectly indicates the leakiness of the blood vessels in the acute stage of a stroke. Several hours after the injection of Gd-DTPA, FLAIR images exhibit the disruption of the BBB, which appears as an enhancement in the sulci over the infarcted area in 1/3rd of acute ischemic stroke patients (31). BBB damage is an important factor in the growth of ICHs and hemorrhagic transformations (303233). The permeability of the BBB can increase in acute strokes because of the breakdown of the BBB by the ischemic insult. The BBB breakdown can potentially explain the mechanism underlying the damage to the cerebral vasculature in largeartery stenosis, which causes a chronic ischemic insult to the brain. Therefore, the leakage of blood through the BBB to the subarachnoid space in patients with an ischemic stroke may be possible.
In contrast to many previous studies, our study showed that ischemic stroke is the major etiology of the cSAH. The possible reason for the current results is that the difference in proportionate distribution of ischemic-stroke subtypes between Western and Korean populations. Most previous studies on cSAHs are conducted on Western patients. Furthermore, Western patients have a significantly greater proportion of cardioembolic and cryptogenic stroke, as compared with Koreans (34). The Korean population has a high incidence of cardioembolic stroke but also exhibits the greatest proportion of large-artery atherosclerosis among the ischemic stroke subtypes (35). The higher relative incidence of large-artery atherosclerosis in Korean patients may be one of the reasons why ischemic strokes are frequently associated with cSAHs. Thus, large-artery atherosclerosis may cause a chronic ischemic insult to the brain, which could be the mechanism underlying cSAHs.
Our study had some limitations. Our observations reflect experiences at a single tertiary care center, as obtained by a retrospective analysis. Thus, the study may have sources of selection bias.
In conclusion, ischemic stroke could be a common underlying etiology of isolated acute nontraumatic cSAHs. Damage to the cerebral vasculature, particularly the breakdown of the BBB due to an ischemic stroke, is the possible and dominant mechanism underlying the cSAH.




 XML Download
XML Download