

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Prostate cancer (Pca) has been known as the most common male cancer and the second leading cause of cancer-related death in the United States.1 Although Pca in Korea is not as common as that in the United States, it has also shown a markedly increasing trend.2
External beam radiation therapy (RT) is one of the preferred options for treatment of Pca due to its appropriate balance between disease control and treatment-related toxicity.3 Although a wide variety of RT schemes are available, stereotactic body radiotherapy (SBRT) scheme delivering larger fraction dose is known to be especially effective for localized Pca due to relatively lower radiobiological reaction of Pca than those of other types of cancers.45678 However, because the potential risk of toxicity is inevitably increased in SBRT, a special concern is required for motion tracking for prostate when performing SBRT.9
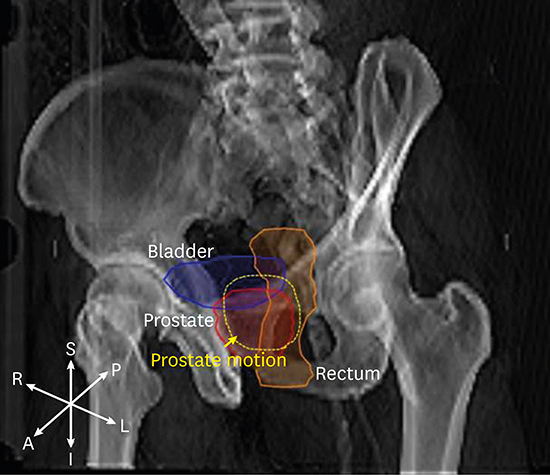
Prostate motion during treatment appears as a form of baseline shift between fractions (i.e., inter-fractional change) or as a momentary position change during treatment (i.e., intra-fractional change).10 Of these two motion types, inter-fractional movement can be easily corrected in actual treatment by applying one or more image-guidance methods.1112131415 However, correction for intra-fractional prostate motion is rather difficult even with current state-of-the-art techniques because correction for this type of motion requires both constant observation and instant adjustment of radiation targeting.
The tumor-tracking method incorporated in CyberKnife (CK) system is a unique technique among commercially available methods in that it provides real-time correction of intra-fractional prostate motion. In this method, the position change of prostate gland is frequently observed using dual X-ray imaging system combined with fiducial insertion scheme.16 In addition, once an error is detected by the imaging system, it can be immediately corrected by precisely adjusting the targeting position using freely movable robotic manipulator. However, the clinical effectiveness of such image-guidance tracking method has not been well understood mainly due to the lack of clinical study on tumor motions. Although several studies have shown how large the prostate motion could occur during treatments, none of these studies have analyzed how the prostate motion the effect to treatment outcome.1718
The objective of this study was to quantitatively analyze the correlation between treatment outcome and prostate motion using clinical follow-up data and prostate motion data acquired at the time of CK SBRT.
METHODS
Patients
Patients who met all of the following inclusion criteria were included in this study: 1) histologically proven prostate adenocarcinoma, 2) radiologically proven localized disease, 3) not severe performance status with Eastern Cooperative Oncology Group (ECOG) performance score between 0 and 2, and 4) no serious comorbidity that could affect treatment outcome. Patients who had any of following conditions were excluded from analysis: 1) lymph node metastasis, 2) distant metastasis, 3) previous history of chemotherapy or radiotherapy, and 4) incompletion of planned radiotherapy. Among those patients who received CK prostate SBRT in our institution between June 2010 and January 2017, 71 patients who fully fulfilled the above inclusion criteria without meeting the exclusion criteria were selected for analysis.
The included patients were assessed for biochemical failure (BF) through laboratory assessment for prostate-specific antigen (PSA) level and toxicity profile based on patients' symptoms and signs. These assessments were carried out on a monthly basis for the first six months after SBRT, every three months thereafter for the first year, and every six months thereafter. Follow-up images for individual patients such as prostate magnetic resonance image (MRI) or bone scan image were normally taken every 6 months after SBRT, but they were taken immediately if any signs of recurrence were found.
CK SBRT
All patients were implanted three fiducial markers using ultrasound guidance into the prostate (two at each sides of base and one at apex of prostate). After the fiducial insertion, computed tomography (CT) images were obtained in supine position with rectal enema and bladder filling. The prostate alone was delineated as gross tumor volume (GTV) for low- to intermediate-risk patients. For high-risk patients, the proximal half of seminal vesicles was added into the GTV along with the prostate. Clinical target volume (CTV) was defined to be the same as GTV. Planning target volume (PTV) was expanded at CTV by 5 mm in all directions except for posterior direction which was expanded by 3 mm for adjacent rectum sparing. Rectum and bladder were delineated as primary organs at risk. Inverse treatment planning method was applied using Multiplan version 3.5.4 (Accuray Inc., Sunnyvale, CA, USA). The prescription dose was 37.5 Gy in five fractions which was normalized to 78%–84% of the maximum dose so that the entire GTV and at least 95% PTV were covered by the prescription-dose surface. Rectum and bladder were basically constrained to be V36Gy ≤ 1 mL and V37.5Gy ≤ 5 mL, respectively, with VxGy representing the volume receiving more than x Gy. However, if constraints were technically incompatible with target coverage requirements, V36Gy ≤ 3 mL (rectum) and V37.5Gy ≤ 10 mL (bladder) were compromised as acceptable.19
Prostate motion measurement
Position of prostate was basically observed using a pair of orthogonal planar X-ray images taken at 45° and 135° with respect horizontal direction. Because the prostate cannot be seen directly in planar X-ray image, there must be surrogate marker reflecting the position of prostate gland. In this study, three gold fiducials with 3-mm length and 0.9-mm diameter were used as surrogates. They were inserted at least one week before the planning CT scanning. Position change in the prostate relative to its original position in planning CT scan was then estimated by comparing the positions of gold fiducials between digitally reconstructed radiographies from planning CT scan and live X-ray images acquired at the time of treatment.
Between two types of prostate motion during CK-based SBRT, inter-fractional position change of prostate could be eliminated almost completely by repeatedly matching observed marker positions to planned positions, leaving only the intra-fractional prostate movement as a meaningful motion in the tumor-tracking prostate SBRT.
The intra-fractional movement of prostate was measured discontinuously using in-tempo imaging method incorporated in the CK system. In this method, the imaging interval was automatically adjusted by the detected motion magnitude. If the movement was increased to 3 mm, the imaging was taken at every beam delivery. If the motion was stabilized below 1 mm, the measurement interval was stretched to 8 beam intervals. On average, the measurement was performed at 5–8 beam intervals in our treatments. Thus, daily intra-fraction motion data consisted of 18–30 movement series since the treatment plan was generally composed of 150–180 beams. Individual movements were measured and recorded along three translational axes (superior-inferior [SI], right-left [RL], and anterior-posterior [AP] axes), from which overall radial magnitude of prostate motion was computed as  , with δx representing a magnitude of prostate motion along x axis.
, with δx representing a magnitude of prostate motion along x axis.
, with δx representing a magnitude of prostate motion along x axis.For statistical analysis, it is beneficial to transform these series of intra-fractional movements into a single representative value. The relationship of van Herk et al.20 could be the first theoretical background for this transformation. In the relationship, the optimal margin was determined to be 2.5Σ + 0.7σ, with Σ and σ representing the average value and standard deviation of motion series, respectively. This relationship indicated that the fluctuated motion around the baseline had 0.7/2.5 times less impact in dosimetric change than average baseline shift. Based on this rationale, the effective magnitude of intra-fractional motion (Deff) was defined by adding weighted fluctuated prostate motion into the average shift and expressed as Σ + (0.7/2.5)σ. Unless otherwise specified, the magnitude value for intra-fractional movement written throughout the paper means Deff.
Statistical analysis
Local recurrence (LR), BF, and late treatment-related toxicity were statistically evaluated for intra-fractional tumor motion detected at each fractional treatment. LR was defined as reappearance of tumor within or adjacent prostate region judged by a radiologic image examination. BF was defined based on the Phoenix definition of PSA failure (i.e., PSA increment of more than 2 ng/mL from nadir). In this definition, the date of BF failure was determined as the time of the first BF detection.21 Treatment-related toxicities on rectum and bladder were assessed through follow-up evaluation by qualified physicians based on the Common Toxicity Criteria for Adverse Events version 4.03. Biochemical failure free survival (BFFS) duration was defined as the duration between the end of SBRT to the date of BF. BFFS was estimated using the Kaplan-Meier method. Log-rank test was used to calculate statistical significance between different survival curves. Univariate logistic regression analyses were conducted to identify potential predictors of LR, BF, and toxicities to rectal and bladder. Receiver-operating characteristic (ROC) curves associated with intra-fractional tumor motion were generated to evaluate the predictive ability of rectal and bladder toxicities and determine the cutoff level for predicting the development of rectal and bladder toxicities. All analyses in the study were performed using SPSS software version 21.0 (SPSS, Inc., Chicago, IL, USA). A P value < 0.05 was considered statistically significant.
RESULTS
Patient characteristics
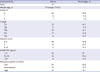
Patient characteristics and clinical workup results are summarized in Table 1. For the total of 71 patients enrolled in this study, their median age was 75 years (range, 53–87 years). Their ECOG performance scores were 0 (62 patients), 1 (8 patients), and 2 (1 patient), and all of them tolerated the full course of SBRT. Three different risk values (low risk, intermediate risk, and high risk) were assigned to these enrolled patients, considering to each T stage, Gleason score, and initial PSA levels based on the National Comprehensive Cancer Network (NCCN) criteria. For T-stage, the risk values were given according to the criteria of T1, T2, and T3 stages, respectively. In our patients, 32 patients had T1 stage (all with T1c), 30 had T2 stage (8, 10, and 12 patients had T2a, T2b, and T2c stages, respectively), 9 patients had T3 stage (all with T3a), resulting in that a total of 61 patients (87.3%) had T1- to T2-stage tumors localized only within the prostate gland without invasion into seminal vesicle or nearby organs. Risk values associated with the Gleason score were assigned into the following three criteria: ≤ 6, = 7, and ≥ 8. Of these patients, 48 had Gleason score ≤ 6, 14 had Gleason score = 7, and 9 patients had Gleason score ≥ 8. Risk value associated with initial PSA level was also assigned with three criteria: PSA level (ng/mL) < 10, 10–20, and > 20. A total of 44, 18, and 9 patients had PSA levels < 10, 10–20, and > 20 ng/mL, respectively. Individual patients were then grouped into three (low, intermediate, and high risk groups) by taking the highest risk value of either T-stage, Gleason score, or initial PSA as recommended by NCCN guideline. As a result, 20 (28.2%), 41 (57.7%), and 10 (14.1%) patients were assigned into the low-, intermediate-, and high-risk groups, respectively.
Table 1
Patient characteristics and initial work-up results
Six (8.5%) patients were subjected to androgen deprivation therapy prior to SBRT.
Clinical results
The median follow-up duration was 47 months (range, 3–79 months). During follow-up, PSA level was initially decreased after SBRT in all patients, but ultimately increased in some patients, with 3 (4.2%) patients showing LR and 12 (16.9%) patients showing BF. Seven patients died during the follow-up period. BF in 7 of 12 patients developed within 3 years after SBRT, resulting in an overall 3-year BFFS rate of 88.2%.
Treatment results including overall death, LR, and BF were analyzed separately for low- to intermediated-risk and high-risk groups. In low- to intermediate-risk groups, treatment failures due to death, LR, and BF occurred in 6 (9.8%), 1 (1.6%), and 6 (9.8%) patients, respectively. However, in the high-risk group, these occurred in 1 (10%), 2 (20%), and 6 (60%) patients, respectively. Treatment-related toxicity after SBRT was common so that more than half of our patients experienced it, particularly on their rectum and bladder. However, the severity of toxicities was usually mild and transient. Regarding rectal toxicity, 30 (42.3%) of 71 patients had grade-I toxicity with mild rectal discomfort or bowel habit changes, 17 (23.9%) patients had grade-II toxicity with persistent anal pain or transient rectal bleeding, and 5 (7%) patients had grade-III toxicity with rectal fistula or intervention for hemostasis. Regarding bladder toxicity, 30 (42.3%) patients had grade-I toxicity with minimal increase in frequency, urgency, or dysuria, 17 (23.9%) patients had grade-II toxicity with moderate increase in frequency, urgency, or dysuria, and 5 (7%) patients had grade-III toxicity with gross hematuria. A total of 52 and 52 patients had adverse side effects in their rectum and bladder, respectively. Of which each 22 patients had grade-II or worse side effects in one of the two organs.
Treatment-related toxicity was also separately analyzed by risk groups. In the low- to intermediate-risk groups (n = 61), 17 (27.9%) and 20 (32.8%) patients had grade-II or worse side effects in the rectum and bladder, respectively. In the high-risk group (n = 10), 5 (50%) and 2 (20%) had grade-II or worse side effects in the rectum and bladder, respectively.
Intra-fractional target motion
Fig. 1 shows population histogram of effective magnitude (Deff) of intra-fractional prostate movements for 71 patients examined. The histogram showed that most Deff were distributed within 1 mm in any translational axis, indicating that the intra-fractional movement was generally not large compared to treatment planning margin (3–5 mm). Only 2 (2.8%), 1 (1.4%), and 15 (21.1%) patients had Deff exceeding 1 mm in SI, RL, and AP axes, respectively. In addition, no patient had Deff exceeding 2 mm in any translational axis. When only scalar magnitude of the movement was analyzed without considering directionality (i.e., radial magnitude shown in Fig. 1D), 32 (45.1%) and 1 (1.4%) patients showed movements larger than 1 mm and 2 mm, respectively. Average magnitudes of effective intra-fractional movements along SI, RL, and AP axes were estimated to be 0.15 mm ± 0.31 mm, 0.12 mm ± 0.19 mm, 0.73 mm ± 0.32 mm, respectively, in mean ± standard deviation format. The overall radial magnitude of the motion was found to be 1.0 mm ± 0.35 mm.

Clinical results with prostate motion
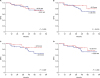
The correlation between clinical results and intra-fractional movement was analyzed. Regarding disease-control related outcomes such as LR and BFFS, it was found that the intra-fractional movement in any axis was not a significant predictive factor for LR or BFFS. These results are summarized in Table 2 and displayed in Fig. 2 as a function of BFFS rate with Deff. In sharp contrast, rectum and bladder toxicities were strongly correlated with intra-fractional movement in specific directions. As shown in Table 2, the incidence of grade-II or worse rectal toxicity was significantly associated with motion along the AP axis (P < 0.001). It was also significantly associated with radial magnitude (P < 0.001). In addition, the incidence of grade-II or worse bladder toxicity was also significantly associated with motion along the AP axis (P = 0.018).
Table 2
Relationship of intra-fractional tumor motion with LR, BFFS, and grade-II or worse rectal and bladder toxicities
Fig. 2
Relations of BFFS with intra-fractional movements along (A) SI, (B) RL, and (C) AP directions, and (D) overall RA motion.
BFFS = biochemical failure free survival, SI = superior-inferior, RL = right-left, AP = anterior-posterior, RA = radial.
In order to make further clear the association of prostate motion with treatment-related toxicity, we performed the similar analysis with grouping the patients as low-, intermediate-, and high-risk groups based on T-stage, Gleason score, and PSA level as recommended in NCCN guideline. The results are summarized in Table 3 and showed that the prostate motion during treatment could be the significant risk factor to increase the rectal and bladder toxicities in each risk group, though it was not statically clear in the high-risk group due to its small patient number.
Table 3
Association of intra-fractional tumor motion with rectal and bladder toxicities in low- to high-risk patients grouped according to the NCCN guideline
| Risk group | Motion | Rectal toxicity | Bladder toxicity |
|---|---|---|---|
| Low risk | AP | P < 0.001 | P < 0.001 |
| RA | P = 0.038 | NS | |
| Intermediate risk | AP | P < 0.001 | P < 0.001 |
| RA | P = 0.040 | NS | |
| High risk | AP | P < 0.001 | P < 0.001 |
| RA | NS | NS |
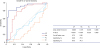
ROC curves are plotted along each translational axes (Fig. 3) to predict the development of grade-II or worse rectal or bladder toxicities in relation to intra-fractional movements. Relative areas under the curves became the largest under the AP-axis ROC curve (at 0.888, P < 0.001). The next largest was at 0.774 (P < 0.001) under the radial-magnitude curve as summarized in inset table of Fig. 3. We determined the cut-off value for intra-fractional movement as the value that maximizes the sensitivity and specificity in the ROC curves. The cut-off value of magnitude in AP motion for the development of grade-II or worse toxicity was determined to be 0.73 mm (sensitivity of 80.6% and specificity of 94.3%). Of the total of 71 patients, 33 showed motions over 0.73 mm along the AP direction, of which 29 (87.9%) experienced grade-II or worse toxicity. If excluding these 33 patients, the incidence rate of grade-II or worse toxicity was decreased to 18.4% (7 patients). The same analysis was applied for radial magnitude of motion. The cut-off magnitude for grade-II or worse toxicity was determined to be 0.92 mm (sensitivity of 77.8% and specificity of 74.3%).
Fig. 3
ROC curves for prostate motion along three translational axes (AP, RL, and SI) and overall radial magnitude to predict grade-II or worse rectal and bladder toxicities. The straight diagonal line on which the sensitivity is equal to 1 in specificity is drawn for reference. Statistical analysis results related to the graph are shown in the inset table.
ROC = receiver-operating characteristic, AP = anterior-posterior, RL = right-left, SI = superior-inferior, RA = radial.
DISCUSSION
The aim of this study was to quantify the relationship between treatment outcome and prostate motion using clinical follow-up data and prostate motion data acquired at the time of CK SBRT. To achieve this purpose, we first analyzed magnitude distribution of intra-fractional movements in prostate SBRT extracted from actual treatment logs. This analysis regarded the prostate motion as significant when Deff was greater than 2 mm by taking into account the following facts: first mechanical error of CK equipment, which was independent of patient, was generally allowed up to 1 mm and second, the sum of all possible errors, including patient-independent and patient-dependent errors, must be smaller than treatment planning margin (3 mm in posterior direction in this study). The analysis result shown in Fig. 1 revealed that the intra-fractional motion was less than 2 mm in all patients except for one who had 2.20 mm on the basis of radial magnitude, indicating that intra-fractional movement was generally much smaller compared to the planning margin used in the current protocol of prostate SBRT (3 to 5 mm).
Intra-fractional prostate motion has been controversial. Some studies have reported considerable amount of prostate movements requiring mandatory correction, while other studies have reported only negligibly small movements.1622232425 If only considering the magnitude alone, our results seem to support the latter, but actually did not so if it was analyzed in more detail including the treatment outcome. This will be discussed in more detail below.
Next, we analyzed how intra-fraction motion affected treatment outcome in tumor tracking SBRT for Pca. Treatment outcome was evaluated in both aspects of tumor control and toxicity. The former was assessed primarily based on 3-year BFFS rate while the latter was based on rates of toxicity to bladder and rectum. The overall 3-year BFFS rate was estimated to be 88.2% in Kaplan-Meier method analysis with 7 cumulative BF events occurred within 3 years. This ratio of BFFS was lower compared to those reported in previous studies (93.0%–93.9%) for CK-based SBRT for Pca.1926 This discrepancy might be due to the fact that the present study included some high-risk patients (10 patients), unlike the previous studies. In fact, if these high-risk patients were excluded, the BFFS rate (94.4%) became very similar to those previously reported values, suggesting that our treatment quality was not significantly different from those of previous CK-based prostate SBRT.
The BFFS was further sub-analyzed for magnitude of intra-fraction movement in order to reveal tumor-tracking efficacy in aspect of tumor control. The BFFS showed only tiny differences with magnitude of intra-fractional movement in all axes as shown in Table 2 and Fig. 2, indicating no significant correlation of BFFS with intra-fractional movement. However, the incidence of side effects on nearby organs was clearly related to intra-fraction movement. More interestingly, such the incidence of side effect had a clear directional dependence on intra-fractional movements. The intra-fractional movement in AP direction was significantly associated with both the incidence of rectum (P < 0.001) and bladder toxicities (P = 0.018), which were remarkably increased when the movement was increased over the referenced cut-off value of 0.73 mm as shown in Table 2. The overall radial magnitude of intra-fractional movement was also significant associated with rectal toxicity. However, this radial motion was not significantly associated with bladder toxicity. On the other hand, movements in RL and SI directions did not show any correlation with rectum or bladder toxicity.
These contrasting features of intra-fractional movement between tumor control and treatment-related toxicity can be explained as follows. First, the non-relationship between intra-fractional movement and local-tumor control might be due to the fact that the intra-fractional movement was not large enough to affect local-tumor control in our patients. Although real-time error correction system in CK can eliminate targeting error in principle even when intra-fractional movements are significantly larger as presented in previous phantom studies, this could not be confirmed with the current motion data alone due to the relatively smaller magnitude distribution (Fig. 1).2728 Second, increased toxicities to rectum and bladder with increasing intra-fractional movement indicated that doses actually delivered to these organs were also increased in proportion to intra-fractional movement. Although the intra-fractional motion error was corrected by the tumor-tracking system in CK, some residual error inevitably remained. Such residual error might have been increased in proportional to the magnitude of intra-fractional motion. Our results strongly demonstrated that treatment-related toxicity was very sensitive to this kind of small residual errors, unlike local tumor control rate. Considering that the bladder and rectum are located anterior and posterior to the prostate, respectively, it can be easily understood that rectum and bladder toxicities are particularly sensitive to AP-directional motion of the prostate.
Finally, we attempted to present the tolerance magnitude of the intra-fractional movement regarding combined toxicity on both rectum and bladder using ROC analysis method. In this analysis, the magnitude of the tolerance was determined as the cut-off value at which the difference between the incidence rates of grade-II or worse toxicity with intra-fraction movements smaller and greater than the cut-off value was maximized. The analysis result showed that AP-directional and radial magnitudes of intra-fractional motions were significant at tolerance magnitudes of 0.73 and 0.92 mm, respectively. Particularly, the AP directional movement was sensitive (80.6%) and specific (94.3%) enough to be used as a prognostic factor for treatment-related toxicity on rectum and bladder. For example, if AP motion exceeds the tolerance limit (0.73 mm), it can be considered as a signal to apply adaptive re-planning for further rectum and bladder sparing.
To the best of our knowledge, this is the first clinical study that analyzes treatment outcome related to target motion in prostate SBRT. However, this study does have some limitations. First, this study was limited by its retrospective nature. Second, patients who received neoadjuvant hormone therapy and high-risk Pca patients were included. This could result in some distortion in statistical analysis of results. Third, there was no comparison with different types of SBRT other than tumor-tracking SBRT. Fourth, this study did not include dosimetric parameters related to toxicities. Furthermore, the follow-up duration was not long enough. Therefore, prospective, comparative, and long-term follow-up studies are needed to confirm our results.
In conclusion, intra-fractional prostate movement was found to have significant correlation with treatment-related toxicity, but not with tumor control, in tumor-tracking SBRT for Pca. Particularly, AP-directional movement showed a strong correlation with treatment-related toxicity. It resulted in a rapid increase in toxicity with only a slight increase over referenced tolerance of 0.73 mm. Our results re-emphasize that, no matter how small it may seem, robust fixation and precise correction are strongly required in prostate SBRT.
 XML Download
XML Download