

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Migraine is a prevalent, debilitating neurological condition that lacks a universally effective therapy. It is characterized by attacks of throbbing, unilateral pain associated with nausea, vomiting, phonophobia, and photophobia [1].
1. Current treatments of migraine
Migraine treatment in emergency departments presents a clinical appeal for both patients and health care providers. Patients' response to medications is widely idiosyncratic and treatment agents that were effective in one patient might fail in another apparently similar case. Therefore, the treatment must be tailored to each individual case. The mainstays of current migraine management options include non-steroidal anti-inflammatory drugs (NSAIDs) and triptans [2]. NSAIDs are used for mild to moderate attacks of migraine as well as acetaminophen, which is proven to be effective for attacks of moderate severity [34]. Unfortunately, NSAIDs have a short half-life; therefore, repeated administration may be needed on a single attack of migraine and adverse effects like tight throat and flushing are common [56]. Triptans are usually prescribed for severe attacks not responding to the NSAIDs/acetaminophen strategy [5]. However, the associated side effects limit their prescription in the clinic. The combination of analgesics with tramadol, barbiturates, or stronger opioids, like morphine, is restricted to exceptionally unresponsive cases. Thus safer, more tolerable, and mechanism-based treatment approaches for migraine are imperative.
2. Magnesium sulfate for migraine
Suboptimal magnesium level has been repeatedly reported in migraine patients [789]. Consequently, several clinical trials investigated the efficacy and safety of parenteral and oral magnesium supplementation in acute migraine [1011121314]. Some studies support the use of oral magnesium for the prophylaxis of migraine [15].
3. Intravenous caffeine for migraine
Caffeine has been recommended for acute migraine treatment for hundreds of years [16]. Combinations of caffeine with non-opioid analgesics, ergotamine and codeine showed an abortive effect in acute episodes of migraine [171819]. In two recent trials, we reported that intravenous caffeine has comparable efficacy to ketorolac for ameliorating migraine pain [2021].
There is scarce data on the efficacy of intravenous caffeine citrate for reducing pain scores in patients with acute migraine. We have done some studies about the role of caffeine for pain management in acute migraine headache [16]. We have assessed its efficacy as a sole treatment and also compared it with ketorolac [2021]. To the best of our knowledge, there is not any study that uses intravenous caffeine in this regard, except for those belonging to Baratloo et al. [2021]. To further these investigations, in the current study, we performed prospective research to assess the efficacy of intravenous caffeine citrate vs. magnesium sulfate for management of acute migraine headache.
MATERIALS AND METHODS
1. Study design and setting
This was a prospective quasi-experimental study that was conducted from January until May 2016 in two educational medical centers at Shahid Beheshti University of Medical Sciences (Shoahadaye Tajrish Hospital and Imam Hossein Hospital), Tehran, Iran. Patients with a chief complaint of moderate to severe headache presenting to the emergency department were considered for this study. For patient enrolment, we used the same strict inclusion and exclusion criteria reported in our previous pilot study [21].
2. Definition
The visual analog scale (VAS) is a measurement tool used to quantify the pain score. VAS is a continuous scale comprised of a horizontal or vertical line, usually 10 centimeters (100 mm) in length. In the current study we considered 10 as the highest possible VAS score. In this measurement scale, “no pain” was defined as a score of 0 and “pain as bad as it could be” or “the worst imaginable pain” was considered as a score of 10 [22].
3. Study population
Patients who referred to the emergency department were deemed eligible and included in the study if they met the following criteria: 1) their age ranged from 18 to 60 years old; 2) their complaint of migraine pain fulfilled the criteria of a common migraine based on the International Headache Society Criteria and they had had migraines for at least a year prior to the admission day [1]; and 3) their VAS pain score indicated severe or moderate pain (VAS pain score ≥ 4) [2324].
We excluded patients who had, at least, one of the following items: 1) a history of any cardiac dysrhythmia; 2) hypertension; 3) ischemic heart disease; 4) active peptic ulcer disease; 5) inflammatory bowel disease; 6) pregnancy; 7) were breast feeding; 8) coagulopathy; 9) renal failure; 10) hepatic failure; or 11) a sleep disorder.
The sample size was calculated to detect a change of at least 3 cm in the VAS scale; considering β = 0.01 and α = 0.05, the minimum sample size for the study was estimated to be 35 subjects in each group.
4. Intervention
Those presenting to the emergency department of Shohadaye Tajrish Hospital received a 60 mg caffeine citrate intravenous infusion within about 10 minutes. Those referring to the Imam Hossein Hospital received an intravenous infusion of 2 g magnesium sulfate. Both drugs were diluted in 100 cc normal saline 0.9% and infused over 10 minutes. All patients were monitored for any possible side effects. If any adverse effects (tachycardia, hypertension, itching, nausea and vomiting, pain at the injection site, irritability) happened, the process had to be stopped. At one and two hours after drug administration, patients were asked about their pain score on the VAS scale. A decrease of more than 3 points on the pain scale was considered a proper response [25].
5. Statistical analysis
Statistical analysis was performed using SPSS version 22. For describing continuous variables and mean, standard deviation, median, and inter-quartile range were used. The Chi-Square test and student t-test were used for analysis of baseline characteristics. The Mann-Whitney U test and Wilcoxon signed rank test were used to analyze differences in VAS pain scores. A P value ≤ 0.05 was considered significant.
6. Ethical considerations
The study was performed with a strict commitment to ethical considerations of the Declaration of Helsinki. All eligible patients were informed about the new drug, and all gave a signed informed consent. The study protocol was approved by the ethical committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran. This study is registered in the Iranian Registry of Clinical Trials (www.irct.ir) under the code IRCT2016061315640N2.
RESULTS
Seventy patients were enrolled in the study. Their mean age was 33.1 ± 11.3 years. Forty-five of the patients (64.3%) were female and 25 (35.7%) were male. Baseline characteristics of the patients in the two groups are shown in Table 1. Age and gender were significantly different in the two studied groups.
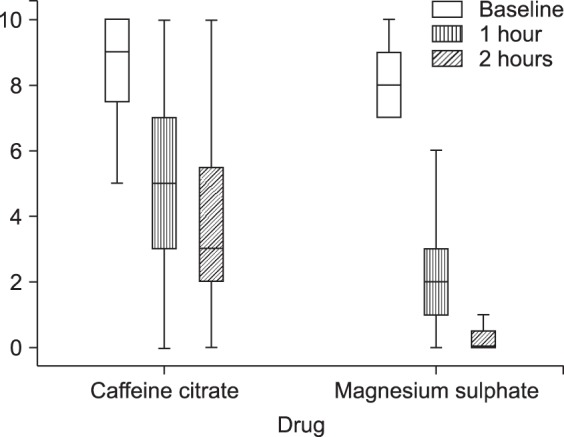
For the Caffeine citrate group, the median (interquartile range (IQR)) of the VAS pain score decreased significantly from 9.0 (2.0) to 5.0 (4.0) after one hour and to 3.0 (4.0) after two hours. For the Magnesium Sulfate group, the VAS pain score decreased significantly from 8.0 (2.0) to 2.0 (2.0) after one hour and to 0.0 (1.0) after two hours (Fig. 1).
The VAS pain score decreased more in the Magnesium sulfate group compared to the Caffeine citrate group after one hour (P < 0.001) and two hours (P < 0.001).
DISCUSSION
1. Major pathophysiology of migraine
Headache is the most important and most common manifestation of migraine. Due to the pulsating nature of the headache, the pathophysiology of migraine was attributed to vascular problems in the brain for many years. The vascular theory for explaining migraine, which was considered valid until the middle of the 20th century, was based on 3 observations: 1) observations reported by 2 researchers named Ray and Wolff during a neurosurgical operation on a conscious patient in 1940; 2) inflation of carotid and extracranial arteries and seeing them pulsating during migraine headache attacks; 3) effectiveness of ergotamine, which is a powerful vasoconstrictor, for treating migraines [2627]. Currently, previous theories are questioned and more thorough investigations are being carried out on this topic. Modern imaging methods have shown that changes in vascular diameters are not proportionate with pain severity and response to treatment [28293031]. It seems that at the beginning of the headache vasodilation has not occurred yet, raising the question about the role of vasodilation in the pathophysiology of this disorder [32]. Therefore, migraine is not a primary vascular event and it seems that stimulation of trigeminal nerve branches as well as parasympathetic nerves following a series of activities in the brain's cortex (cortical spreading depression) leads to reactions in the meninges and brain stem that can explain migraine symptoms [33]. Disorders in the function of aminergic brain stem nuclei result in vasodilation and an increase in severity of pain through a series of reactions, and vasodilation brings about other neurogenic reactions. The close relationship of the vessels in the meninges with the trigeminal nerve branches helps in a better understanding of these events [34].
2. Efficacy of studied agents
The results of this study showed that both intravenous magnesium sulfate and intravenous caffeine citrate could be considered for treatment of acute migraine headache. However, magnesium sulfate caused a more significant reduction of the VAS pain score compared to caffeine citrate at one and two hours after administration. However, there was a significant difference in age and sex between the studied groups that could be “confounding factors”.
3. Safety of treatment
There were no cases of withdrawal or intolerance to the treatment, which indicates the safety of intravenous caffeine citrate and magnesium sulfate in the studied population. There was not any serious adverse event in the studied population throughout the duration of hospitalization. However, this should be interpreted cautiously due to the short period of observation and the strict inclusion and exclusion criteria for selecting eligible subjects.
4. Explanation of results
The molecular mechanism behind migraine has not yet been understood. However, the literature suggests multiple underlying mechanisms, which allows for testing a wide range of therapeutic options. Magnesium deficiency is hypothesized to be implicated in the pathophysiology of migraine. Physiologically, magnesium inactivates excitatory N-Methyl-D-aspartate (NMDA) glutamate receptors [35]. Depletion of magnesium drives NMDA-coupled calcium channels towards abnormal opening, which allows increased calcium influx, causing cytotoxicity and leading to neuronal injury secondary to the generation of toxic nitric oxide radicals [36]. Cortical depression is another possible mechanism for initiation of migraine [3738]. Magnesium deficiency affects mitochondrial oxidative phosphorylation and neuronal polarization, resulting in altered mitochondrial metabolism, which is suggested as increasing susceptibility to cortical depression [39]. On the other hand, the neurogenic theory suggests central sensitization or sensitization of the trigemino-vascular afferents of nociceptive neurons as a possible cause of migraine [404142]. Caffeine acts by inhibiting adenosine receptors (A1 and A2) in the brain, which explains its marked effect as an abortive agent in migraine attacks [16434445].
5. Previous studies
A recent meta-analysis of 21 randomized clinical trials (RCT) demonstrated the favorable effects of both intravenous and oral magnesium sulfate supplementation. Intravenous magnesium sulfate reduced acute migraine attacks within 15 to 45 minutes, 120 minutes, and 24 hours after initial infusion, while oral supplementation alleviated the frequency and intensity of the attacks [46].
Caffeine is frequently used in combination with other analgesics. The acetaminophen/aspirin /caffeine cocktail is classified as a level one option for acute migraine attacks by the American Headache Society, whilst the combination of caffeine and ergotamine is listed as level two [2]. We initiated the use of caffeine as monotherapy in a pilot study followed by an RCT comparing intravenous caffeine and ketorolac [2021]. Both regimens showed comparable positive effect in terms of pain relief, therapeutic success, and incidence of adverse events [2021].
6. Age and sex differences in pain and analgesia
Age and sex varied significantly between the groups in this research. The relationship of migraine pain with these characteristics is complicated and confusing. Bolay et al. [47] claimed that the impact of sex on migraine pain varied with age and significant changes were seen in women over 30 years old; but not in men. Sex also influences headache characteristics and migraine-associated symptoms, which vary across age groups, particularly in women. It has been reported that women have lower pain thresholds and tolerance for pain, but a superior capability to differentiate painful stimuli. In addition, sex differences in response to pain treatment have been proposed. Some have attributed such differences to sex hormones [484950]. Age related changes such as hypothalamic-pituitary-adrenal axis dysregulation and autonomic function changes could lead to increased pain sensitivity. On the other hand, some literature suggests that pain perception diminishes in old age. It seems that existing data regarding pain and aging are limited and equivocal and further studies are needed [5152]. Victor et al. [53] assessed age and sex specific patterns of migraine prevalence in 40892 individuals in the United States. Migraine prevalence was 2-fold higher in females (17.5% vs. 8.6%) but showed a dual peaking around the late 20s and 50 years of age in both sexes.
7. Strong points and limitations
Our study has several strong points: patients were diagnosed according to the migraine diagnostic criteria of the International Headache Society and the severity of pain was assessed by the VAS score, which is a common and reliable measure of pain. There are some limitations: (1) the sample size is relatively small and (2) the study did not investigate the long-term efficacy of the drugs. Lack of randomization is the most important disadvantages of quasi-randomized studies [54]. There are statistical differences regarding age and sex between the studied groups that might have caused a bias in this investigation.
8. Implications for future research
In light of the current evidence, we argue that there is no universal agreement on the treatment of acute migraine. Therefore, management of acute episodes should be individualized on a case to case basis due to the highly idiosyncratic effects of available agents. We recommend further well designed RCTs to confirm the findings of this study.

 XML Download
XML Download