

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pneumocystis jirovecii is an opportunistic fungal pathogen that causes Pneumocystis pneumonia (PCP) in immunocompromised patients [1]. PCP diagnosis is based on clinical presentation, radiological manifestation, and microbiological evidence [2]. The microbiological diagnosis of PCP relies on histological and microscopic identification of the ascus and/or trophic forms of P. jirovecii from respiratory samples using different stains, such as Giemsa, calcofluor-white, toluidine blue O, and Gomori methenamine silver, direct or indirect immunofluorescence (IF) staining, and β-D-glucan assay [23]. However, microscopy following conventional or IF staining is too insensitive to be reliably used for PCP diagnosis [34]. Various PCR assays, particularly real-time PCR, show improved sensitivity compared with microscopic identification methods [567]. An evidence-based review of molecular assays strongly supports the use of real-time PCR for the diagnosis of PCP, particularly in non-HIV immunocompromised patients [3].
Several commercial real-time PCR assays for molecular diagnosis of PCP have been developed, and a few studies have evaluated their performances [6891011]. The RealStar Pneumocystis jirovecii PCR Kit 1.0 CE (RealStar assay; Altona Diagnostics, Hamburg, Germany) was recently developed and has received Conformit Europe In-Vitro Diagnostic approval [12]. In addition, the AmpliSens Pneumocystis jirovecii (carinii)-FRT PCR kit (AmpliSens assay; InterLabService Ltd., Moscow, Russia) is a well-validated, widely used qualitative real-time PCR assay targeting the mitochondrial large subunit ribosomal RNA gene [8]. We compared the performance of these two assays for detecting P. jirovecii DNA in lower respiratory tract (LRT) samples and according to clinical PCP probability.
METHODS
Study design and clinical samples
This study was conducted at Samsung Medical Center, Seoul, Korea, and was approved by its Institutional Review Board (approval number: 2017-02-151), which waived informed consent from the patients. DNA was extracted from 159 respiratory samples (112 bronchoalveolar lavage [BAL] fluid samples, 37 sputum samples, and 10 endotracheal aspirate [ETA] samples) collected from consecutive patients with respiratory clinical symptoms from November 2015 to March 2016. Patient medical records, including clinical, radiological, and treatment data, were collected retrospectively. Of the 159 patients, 51 (32.1%) had a solid tumor, 45 (28.3%) had a hematologic malignancy, and 21 (13.2%) had undergone stem cell transplantation. A total of 143 and 98 patients had clinical and radiological observations compatible with PCP, respectively. Results of microscopic examination using the Calcofluor-white stain were also collected. Based on the clinical information of each patient, three specialists (a microbiologist and two infectious diseases specialists) independently classified the patients into three categories: clinical, possible, and unlikely PCP. The categories were determined on the basis of the following criteria: (i) compatible clinical symptoms (dyspnea, fever, and nonproductive cough), (ii) underlying immunodeficiency, (iii) compatible radiological findings (chest X-ray or computed tomography findings of interstitial infiltrates), and (iv) response to P. jirovecii-specific treatment. Clinical PCP was defined by the presence of all four criteria in the absence of an alternative diagnosis. This category included both microscopically proven PCP and probable PCP with negative microscopic examination. Possible PCP included patients who met three out of the four criteria with no other cause for pneumonia. Unlikely PCP was defined as the presence of fewer than three criteria. The classification was performed blind to the PCR results.
DNA samples were extracted using the MagNA Pure 96 system (Roche Diagnostics, Mannheim, Germany) with the “Pathogen Universal Protocol” according to the procedure recommended by the manufacturer. Extracted DNA samples were stored at −70℃.
Molecular testing and method comparison
The RealStar and AmpliSens assays were performed in parallel according to the manufacturers' instructions. Briefly, the PCR reaction for the RealStar assay was performed in a total volume of 30 µL (20 µL PCR reaction mixture and 10-µL template DNA). Thermocycling conditions included a two min step at 95℃ followed by 45 cycles of 95℃ for 15 seconds, 58℃ for 45 seconds, and 72℃ for 15 seconds. The assay included an artificial heterologous extrinsic control. The PCR for the AmpliSens assay was performed in a total volume of 25 µL (15 µL PCR reaction mixture and 10-µL template DNA). Thermocycling conditions included a 15 minutes step at 95℃ followed by 45 cycles of 95℃ for 20 seconds and 60℃ for 60 seconds. The human β-globin gene was amplified simultaneously as a heterologous intrinsic control to monitor PCR inhibition. For both real-time PCR assays, amplifications were performed on a CFX96 Real-Time PCR Detection instrument (Bio-Rad, Hercules, CA, USA). Positive fungal template (P. jirovecii DNA) and no-template controls were included in each run. Probes specific for the P. jirovecii and the internal control were labeled with the FAM and JOE fluorophores in the RealStar assay, whereas those in the AmpliSens assay were labeled with JOE/HEX and FAM fluorophores. According to the manufacturer's instructions, a positive test result was defined as a cycle threshold (Ct) ≤35 for the AmpliSens assay, whereas any well-defined exponential amplification in the RealStar assay was considered a positive test result. If the internal control was not amplified, the test was considered invalid. The turnaround time (the interval between PCR reagent set-up and amplification) was similar for both assays (140 minutes for the RealStar assay and 130 minutes for the AmpliSens assay, for 54 samples).
Samples with discordant results between the two assays were confirmed by nested PCR and sequencing according to the protocol described by Tia et al. [13], using two sets of primers (outer primers PJLSUF0 and PJLSUR0 and inner primers PJLSUF1 and PJLSUR1) targeting mitochondrial large subunit ribosomal RNA gene. Amplification conditions for the first round consisted of denaturation at 94℃ for two minutes; 35 cycles of 94℃ for 30 seconds, 55℃ for 30 seconds, and 72℃ for 30 seconds; and a final extension at 72℃ for five minutes. For nested PCR, 25 cycles were performed. Following detection of the 113-bp PCR product by gel electrophoresis and purification of the PCR product, sequencing was performed on an automated ABI Prism 3730 instrument using a BigDye terminator cycle sequencing kit (Thermo Fisher Scientific, Waltham, MA, USA). The primers used for the sequencing reaction were the same as inner primers (PJLSUF1 and PJLSUR1) used for the second round of PCR.
Statistical analysis
Diagnostic performance was compared between the RealStar and AmpliSens assays by measuring positive/negative percent agreement and kappa coefficients with 95% confidence interval (CI). Normality of the data was tested using the Shapiro-Wilk test. Nonparametric Kruskal-Wallis tests with Tukey post hoc tests were applied to compare variability and means across the three clinical categories. Two-sided P<0.05 was considered statistically significant. A Pearson correlation analysis was performed between assay results. All analyses were performed using the VassarStats website (http://vassarstats.net/) and SPSS version 24 (IBM Corp., Armonk, NY, USA).
RESULTS
Comparison of the two molecular assays
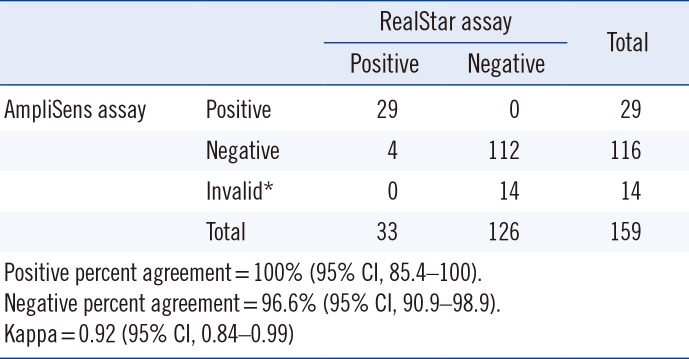
A total of 33 and 29 samples were positive according to the RealStar and AmpliSens assays, respectively. The AmpliSens assay generated 14 invalid results, while the RealStar assay did not generate invalid results. Excluding the 14 invalid results, 145 results were included in the comparative analysis. As shown in Table 1, the two assays showed high agreement rates. Discordant results were observed in four samples, all RealStar-positive and AmpliSens-negative. These were confirmed to be negative using nested PCR followed by sequencing.
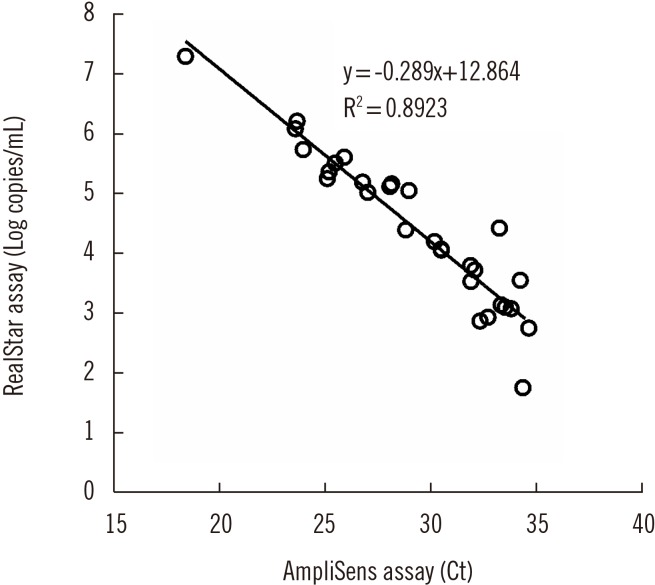
Although the Ct values of the AmpliSens assay without a standard curve could not be interpreted for quantification, a strong correlation was observed between the Ct values of the AmpliSens assay and quantitative results (log copies/mL) of the RealStar assay (Fig. 1).
Patient classification and molecular testing results
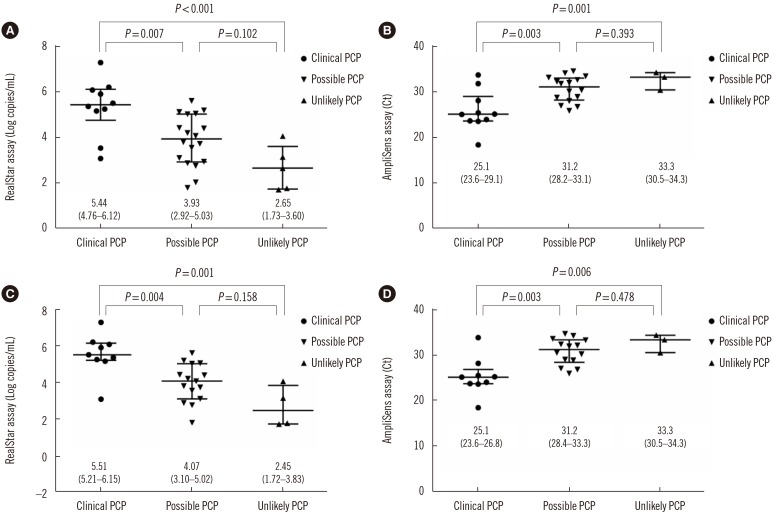
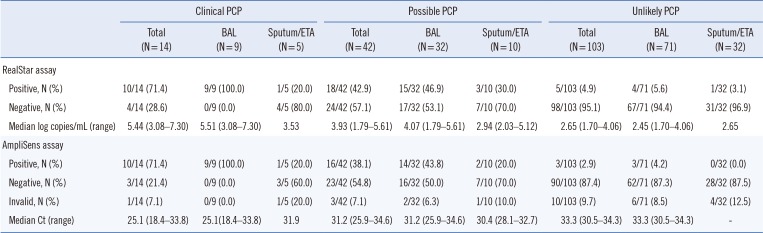
Table 2 presents the number of positive and negative results according to patient classification and sample type. Two BAL fluid samples from patients categorized as clinical PCP were positive by direct microscopic examination using the calcofluor-white stain. In the clinical PCP group, the positive rate in BAL fluid samples was 100% for both assays, whereas only 20% showed positive results in sputum/ETA samples. In the possible PCP group, the positive rate range in BAL and sputum/ETA samples was 43.8–46.9% and 20–30%, respectively. In the unlikely PCP group, the positive rate was <10% for all patients, regardless of the molecular method and sample type. The quantitation results of the RealStar assay and the Ct values of the AmpliSens assay by classification are shown in Fig. 2. Results for both assays differed among the three clinical categories (RealStar assay, P=0.001; AmpliSens assay, P=0.007). P. jirovecii DNA load was significantly higher in the clinical PCP group than in the other groups (Fig. 2A). Similarly, the Ct values were significantly lower in the clinical PCP group than in the other groups (Fig. 2B). For BAL samples, differences were also observed between assay results of the three clinical categories (RealStar assay, P=0.002; AmpliSens assay, P=0.004; Fig. 2C and 2D).
DISCUSSION
Over the past decade, advances in molecular diagnostic testing for detecting P. jirovecii have led to improvements in PCP diagnosis [314]. Numerous studies have shown that PCR assays are more sensitive than non-PCR assays [1516]. However, increased sensitivity can result in false-positive results because of insufficient technical performance or positive results from colonization in addition to infection [317]. These drawbacks for PCP diagnosis can be overcome using quantitative real-time PCR. The closed system of real-time PCR prevents contamination with amplicons, which cause false-positive results. Furthermore, quantification can be used to distinguish true infection from colonization, although an indeterminate zone would remain [314]. In this study, the RealStar assay and the AmpliSens assay demonstrated similar performance. The results of the two assays showed a strong correlation, although the Ct values of the AmpliSens assay could not be used for quantification.
The four samples exhibiting discordant results were positive only in the RealStar assay because of low P. jirovecii burden (<500 copies/mL). This may be explained by differences in data interpretation; a positive test result is defined as a threshold ≤35 for the AmpliSens assay, whereas any amplification in the RealStar assay is considered a positive test result.
The finding that P. jirovecii DNA load was significantly higher in the clinical PCP group than in the other groups shows that real-time PCR can be helpful in discriminating active PCP from colonization. Our data confirm previous findings of a lower fungal burden in colonized patients than in PCP patients [5817181920]. In this context, DNA copy number or Ct values have been suggested as cut-off values of fungal burden for differentiating PCP from colonization [4691721]. However, we did not report cut-off values as the number of patients with clinical PCP was low, and the DNA load distribution of the two assays ranged widely. Our study population comprised non-HIV immunocompromised patients, which could explain the low discrimination level between PCP and other groups compared with studies in HIV-positive patients [4621].
BAL fluid samples provide a good yield for the detection of fungal DNA and are the standard for PCP diagnosis, as P. jirovecii resides mainly in the alveolar space [1]. A gradient of fungal burden is expected between the highest load in BAL fluid samples and the lowest load in upper respiratory tract (URT) samples [3]. Indeed, a few studies have observed higher fungal detection rates in BAL fluids than in URT samples [222324]. However, information regarding the yield obtained from different LRT sample types is limited, particularly in non-HIV immunocompromised patients [2526]. Alanio et al. [26] reported that fungal burdens did not significantly differ between BAL fluids and induced sputum; however, we demonstrated low detection rates from sputum/ETA samples compared with BAL samples. As we used expectorated sputa from non-HIV patients, this difference may be explained by a low DNA burden in sputum/ETA samples. A false-negative result in a sputum/ETA sample can cause PCP diagnosis to be missed, especially in non-HIV immunocompromised patients.
Unlike the RealStar assay, in which no invalid results were observed, the AmpliSens assay gave 14 invalid results. This may be due to differences in the internal controls used in each assay. The RealStar assay uses an artificial heterologous extrinsic control, whereas the AmpliSens assay uses the human β-globin gene as a heterologous intrinsic control to monitor PCR inhibition. As heterologous intrinsic controls monitor the presence of cells and human DNA in a sample, it is possible to assess sample quality as well as nucleic acid extraction and the amplification process [27]. Therefore, these invalid results suggest that the respiratory samples were of inadequate quality.
The present study had some limitations. First, as the samples were obtained from consecutive patients, the number of clinical PCP patients included was low. Second, we could not compare the performance of the two assays with IF or β-D-glucan assays.
In conclusion, the RealStar and AmpliSens assays showed equivalent diagnostic performance. They had high agreement with each other and enabled detection of a low P. jirovecii burden in BAL fluid samples. Thus, both assays may be useful as routine methods for detecting P. jirovecii DNA in a clinical laboratory setting. Nevertheless, low-level PCR positive results should be interpreted while considering clinical context and type or quality of the sample.
 XML Download
XML Download