

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
As hospitals are where elderly patients and those with underlying comorbidities are mainly cared for, a high mortality rate is expected if a coronavirus disease 2019 (COVID-19) outbreak occurs in hospitals. Therefore, strict measures to prevent the spread of COVID-19 in hospital settings are crucial.
There are some guidelines to prevent the spread of COVID-19 in hospitals at the national and international levels.1234567891011121314151617 This study aimed to review whether national and international guidelines provide detailed recommendations to tackle issues with infection control and prevent the spread of COVID-19 in hospitals.
METHODS
We performed a systematic search for controversial issues regarding infection control during the management of patients with COVID-19 in the hospital. Controversial issues and key questions were selected based on discussions with four infectious diseases specialists (B.K., E.S.K., K.H.S., and H.B.K.). The selected issues and subordinate questions are listed in Supplementary Table 1. For the review of domestic and international guidelines, official websites of the World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), European Centre for Disease Prevention and Control (ECDC), and Korea Disease Control and Prevention Agency (KDCA) were screened. Guidelines issued between January 1, 2020, and September 30, 2020, were investigated independently by two researchers (W.J. and B.K.), and contents relevant to the selected issues and subordinate questions were extracted (Supplementary Fig. 1). The reviewed guidelines and their official websites are presented in Supplementary Table 2. The contents were rephrased based on consensus among investigators (W.J. B.K., E.S.K., K.H.S., and H.B.K.).
RESULTS
Infection control measures for the management of COVID-19 patients
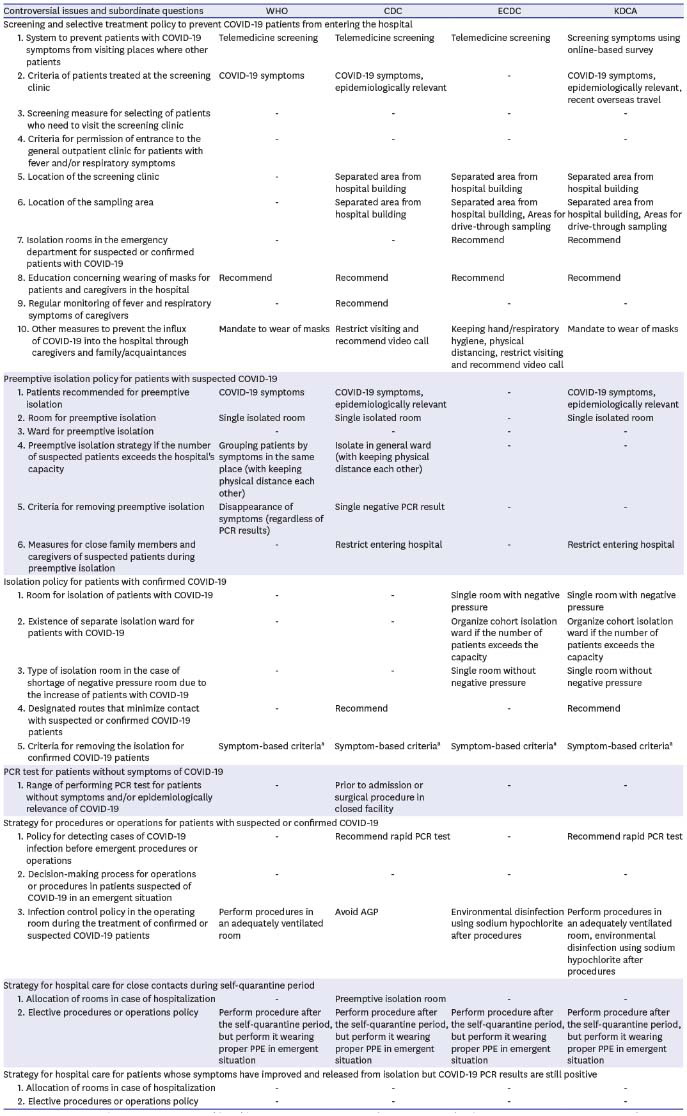
As for screening and selective treatment policies, most organizations recommended that patients with COVID-19 symptoms should be treated at a screening clinic. However, no organization provided recommendations for the type of screening that should be used to identify patients who need to visit a screening clinic, nor did any organization specify criteria for permission to enter the general outpatient clinic for patients with fever and/or respiratory symptoms. All organizations suggested educating patients and caregivers about wearing masks in the hospital.
WHO, CDC, and KDCA recommended a single isolated room for preemptive isolation; however, no organization provided recommendations for determining a specific ward for preemptive isolation. Each organization suggested different criteria for removing preemptive isolation; the disappearance of symptoms was recommended by WHO, a single negative polymerase chain reaction (PCR) result was recommended by CDC, and there was no recommendation by KDCA.
As for an isolation policy for patients with confirmed COVID-19, ECDC and KDCA recommended room requirements for isolation, while WHO and CDC had no recommendations. ECDC and KDCA recommended a single negative pressure room, but they recommended organizing a cohort isolation ward for COVID-19 patients in the case of a shortage of negative pressure rooms. All organizations recommended implementing the symptom-based criteria for removing confirmed COVID-19 patients from isolation.
PCR tests, even for patients without symptoms of COVID-19, were recommended by CDC, while other organizations had no recommendations regarding diagnostic testing. In the case of emergency procedures or operations for patients with suspected COVID-19, CDC and KDCA recommended rapid PCR tests for determining the possibility of COVID-19.
On the strategy for hospital care for healthy individuals who come in close contact with an individual in self-quarantine, only CDC suggested providing a preemptive isolation room for such persons. No organization had recommendations for patients who are released from isolation based on the improvement of symptoms but have consistently positive results from the PCR test (Table 1).
Table 1
Infection control measures for the management of COVID-19 patients
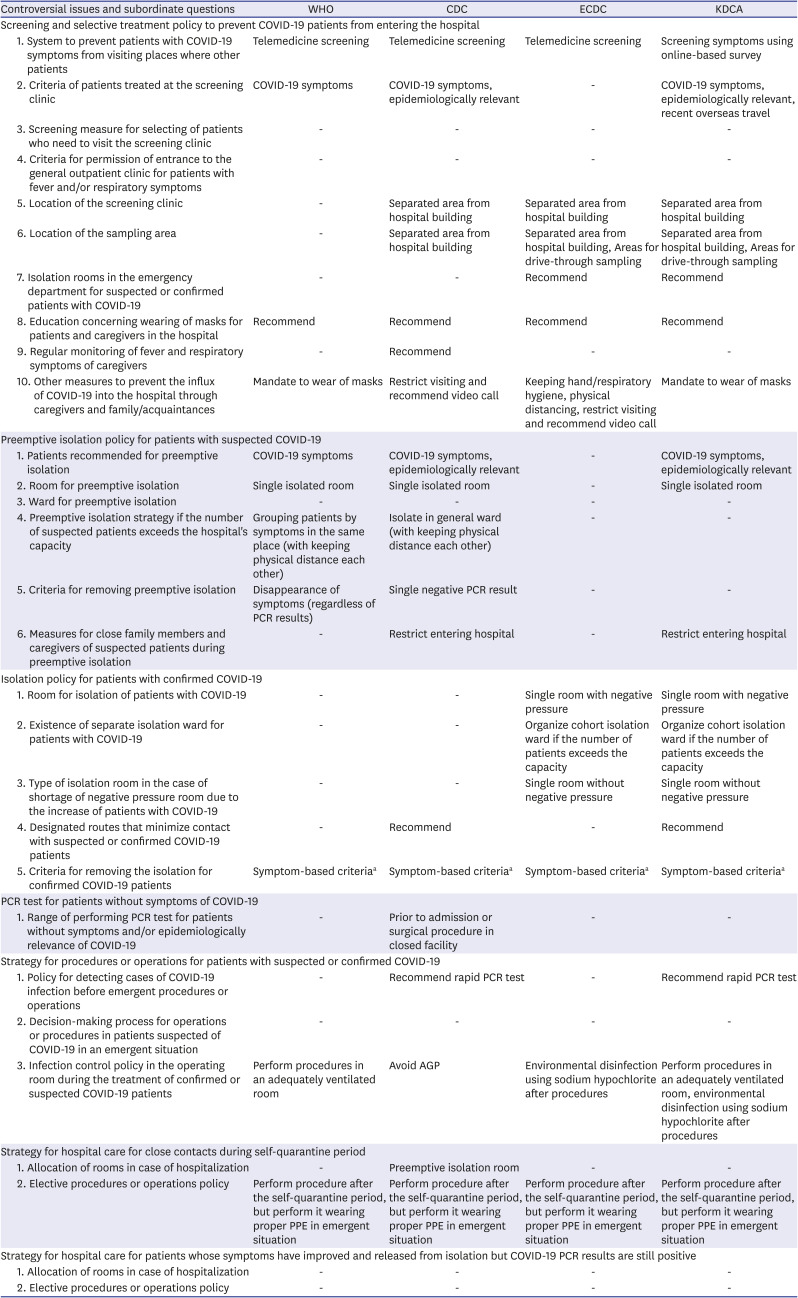
COVID-19 = coronavirus disease 2019, WHO = World Health Organization, CDC = Centers for Disease Control and Prevention, ECDC = European Centre for Disease Prevention and Control, KDCA = Korea Disease Control and Prevention Agency, PPE = personal protective equipment, PCR = polymerase chain reaction, AGP = aerosol-generating procedure.
aSymptom-based criteria for discontinuing transmission-based precautions; - Patients with mild to moderate illness who are not severely immunocompromised: (1) At least 10 days have passed since symptoms first appeared, (2) At least 24 hours have passed since last fever without the use of fever-reducing medications, and (3) Symptoms (e.g., cough, shortness of breath) have improved. - Patients with severe to critical illness or who are severely immunocompromised: (1) At least 10 days and up to 20 days have passed since symptoms first appeared, (2) At least 24 hours have passed since last fever without the use of fever-reducing medications, (3) Symptoms (e.g., cough, shortness of breath) have improved, and (4) Consider consultation with infection control experts. - Patients who were asymptomatic throughout their infection and are not severely immunocompromised: (1) At least 10 days have passed since the date of their first positive viral diagnostic test.
Infection control measures for healthcare workers in hospitals
All four organizations recommended an equivalent level of personal protective equipment (PPE) to treat patients suspected or confirmed with COVID-19: N95/high-level respirator, gown, gloves, and eye protector. Only WHO and ECDC recommended using PPE for the disposal of items from patients with confirmed COVID-19. All guidelines did not consistently recommend disinfection or sterilization of N95/KF94 for reuse. CDC and KDCA provided guidance for disinfection or sterilization of powered air-purifying respirator hoods for reuse.
No organization provided guidance for separating healthcare workers who participate in the care of patients with COVID-19 from those who care for general patients. There were also no recommendations for regular monitoring with PCR tests or chest X-rays or a limit on working hours to prevent excessive workloads for healthcare workers who treat patients with COVID-19. Daily screening using the COVID-19 checklist was recommended in all guidelines.
As for work restriction policies, only CDC provided recommendations for work restriction or PCR tests for healthcare workers who have been in contact with COVID-19 patients or had a fever or respiratory symptoms. The criterion for returning to work for healthcare workers with fever or respiratory symptoms was a single negative PCR test in the CDC guideline.
As for the recommendation for activities outside the hospital for healthcare workers, CDC and ECDC provided some guidance, while WHO and KDCA had no guidance (Table 2).
Table 2
Infection control measures for the healthcare workers in the hospital
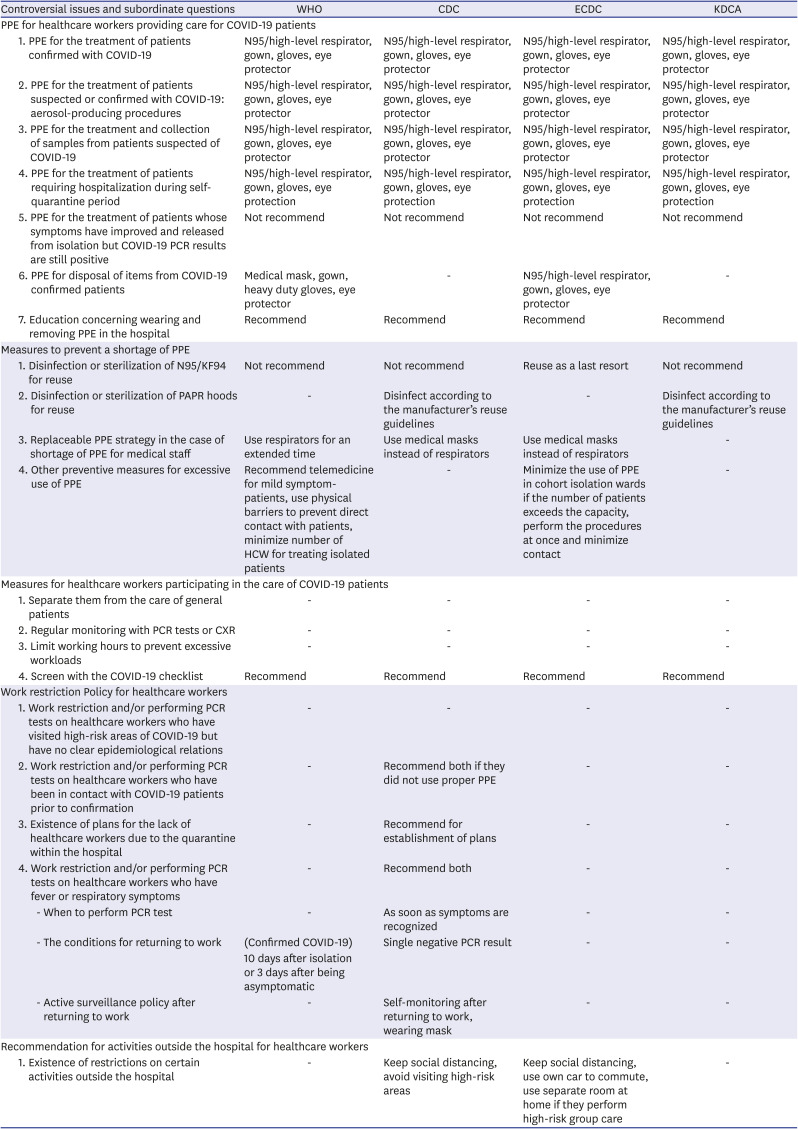
COVID-19 = coronavirus disease 2019, WHO = World Health Organization, CDC = Centers for Disease Control and Prevention, ECDC = European Centre for Disease Prevention and Control, KDCA = Korea Disease Control and Prevention Agency, PPE = personal protective equipment, HCW = health care worker, PAPR = powered air-purifying respirator, PCR = polymerase chain reaction, CXR = chest X-ray.
DISCUSSION
As for the screening and selective treatment policy, there were no guidelines on the criteria for permission to enter a general outpatient clinic. Since the COVID-19 pandemic began, many hospitals have been operating outdoor screening clinics for managing patients with suspected COVID-19 symptoms, such as fever and respiratory symptoms.18 However, screening clinics are equipped with minimal facilities and a workforce that can only provide a minimal examination. Therefore, many hospitals often care for patients with fever and respiratory symptoms who are unlikely to have COVID-19 in the general outpatient clinic because screening clinics have difficulty providing careful evaluation and management. There might be differences among hospitals regarding criteria for permission to enter general outpatient clinics due to the lack of clear guidance on this issue.
A single-center study conducted in South Korea found that 350 suspected COVID-19 cases, defined by symptom and epidemiological associations, were preemptively isolated, and none of them were confirmed with COVID-19.19 Based on the result of this study, both WHO and CDC guidelines, which suggested that isolation can be discontinued if there are no symptoms or if the PCR test is negative, seem appropriate. After all, both WHO and CDC guidelines might be used only in the low possibility of confirmation, such as no close contact with COVID-19 patients.
CDC recommended PCR tests for screening of COVID-19 even for hospitalized patients without COVID-19-related symptoms. The proportion of asymptomatic patients among COVID-19 cases was about 20–30%, and viral shedding also occurred in such patients; there have been concerns about spreading COVID-19 by asymptomatic patients.202122 According to the Infectious Diseases Society of America, the prevalence of COVID-19 among asymptomatic individuals is < 1 to 10%, and considering results of missing a diagnosis of COVID-19 and the sensitivity of the PCR tests, screening for asymptomatic patients is expected to be effective in regions with more than 2% prevalence.23 A study conducted in long-term care facilities in the United States showed that the prevalence of COVID-19 in facilities that performed broad preemptive PCR tests on inpatients was 0.5%, which was significantly lower than 28.0% in facilities that did not perform them.24 This result supports the effectiveness of PCR screening on asymptomatic inpatients.
There were no guidelines for patients who were released from isolation despite a positive PCR test. Although the probability of the existence of infectious severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is very low after 10 days from the onset of COVID-19 symptoms in most cases, patients who are severely ill or immunocompromised could transmit infectious virus particles even after 10 days.2526272829 Therefore, there have been concerns about the possibility of spreading COVID-19 from hospitalized patients who were released from isolation despite a positive PCR test, especially those who need aerosol-generating procedures.28303132 Given that the cut-off values for quantitative RT-PCR and quantitative immunoassays tend to be correlated with infectivity of COVID-19, some researchers have suggested that certain cut-off values could be used as a surrogate marker for the decision to release hospitalized patients from isolation.283334 Further research is needed to determine clear test-based criteria that can guarantee the lack of infectivity of the virus.
Regarding strategies for healthcare workers, there were many recommendations on PPE, but few guidelines for the management of healthcare workers. More specific recommendations are required for patients and healthcare workers because outbreaks in medical institutions could also be spread by medical personnel.35 In addition, there are various reports that healthcare workers in charge of managing patients with COVID-19 are complaining of psychological distress and being exposed to the risk of infection; thus, recommendations to prevent burnout are also needed.3637
There were some potential limitations to this study. Recommendations on key topics might have been updated since then. First, guidelines from only four organizations were reviewed due to linguistic limitations. Second, we reviewed WHO, CDC, ECDC, and KDCA guidelines in September 2020. Even though there have been no critical changes of recommendations on key topics, some significant newly introduced recommendations have been found in revised guidelines until November 2021 (Supplementary Table 3). Given that the average incubation period of COVID-19 is 4 to 5 days after exposure to SARS-CoV-2, CDC currently recommends performing a second PCR test to remove preemptive isolation and return to work for the persons with a higher level of suspicion for COVID-19.38 Moreover, since mRNA vaccines against COVID-19 showed significant efficacy, CDC currently suggests preemptive isolation and PCR tests only for unvaccinated patients if they have no symptoms.39 However, as it has been confirmed that the effectiveness of the vaccine decreases over time, further consideration of the validity period of the vaccine is needed.40
In conclusion, the current guidelines are not yet concrete and uniform enough to be applied to hospital settings, and there is a lack of clear guidelines on controversial vital topics that need to be considered in real medical situations. Therefore, it is necessary to develop recommendations that can be applied to hospital settings after an analysis based on clinical experiences and discussion with experts.
 XML Download
XML Download