

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The persistent increase in the prevalence and incidence of Chronic Kidney Disease (CKD) is a major public health problem worldwide, imposing a significant burden on patients and the healthcare system. Patients with CKD are confronted with a variety of physical and psychosocial problems due to complicated therapies, multiple complications, side effects, and difficulties in recovery [1]. When appropriate intervention is performed, patients with CKD can improve their Quality of Life (QOL) and prolong their survival time [23]. In addition to medical management, the self-management of patients themselves is important before serious symptoms appear. If neglected, the risk of various complications is high [4]. However, when a CKD occurs, in addition to physical problems, psychological and economic problems become burdensome [5]. Therefore, it is difficult for patients to actively try to prevent their deterioration or maintain their health.
Previous studies have suggested that lifestyle modifications are necessary for delaying the progression of kidney failure, reducing complications, and improving QOL [6]. The success of lifestyle modifications in managing CKD depends on the compliance of patients with self-management strategies. Self-management education is the most cost-effective preventive approach to CKD, as it facilitates compliance with treatment regimens and self-management plans. However, self-management education is often limited to the provision of disease-specific information or uses a non-interactive educational approach due to time and manpower restraints in clinical settings [7]. Many patients with CKD are overwhelmed by the practical issues that they need to consider and/or grow frustrated with the significant restrictions and perceived barriers involved with adhering to daily health behaviors. This suggests that rather than simply delivering information to patients, they need to be empowered to make their own decisions and take appropriate actions for managing their health. Moreover, because the day-to-day reality of the condition and circumstances of patients vary considerably, education programs should be appropriately individualized.
CKD is classified into five stages according to the estimated Glomerular Filtration Rate (eGFR). If self-management is successful in stages 2 to 4-that is, before stage 5 or End-Stage Renal Disease (ESRD)-the current state of health may be maintained and the occurrence of ESRD delayed [8]. Since the health of patients with CKD cannot be fully restored once they start renal replacement therapy, it is very important to maintain the current health status of patients with stage 2~4 CKD to prevent conditions requiring renal replacement therapy.
Several studies have shown that individualized empowerment interventions are effective for patients with ESRD [910]. That is, there is an increased likelihood of patients engaging in self-management through empowerment programs. Moreover, an association has been identified between higher perceived self-efficacy scores and QOL [10], as well as increased communication, partnership, self-care, and medication-adherence behaviors [11] after empowerment programs. However, little research has focused on determining the possible effects on patients with CKD between stages 2~4.
The empowerment of patients with CKD is a model of intervention used to facilitate goal-setting ability, problem-solving, stress management, social support, and motivation [12]. More specifically, patients who tend to neglect self-management must strengthen their ability to manage their disease and life. Such patients often tend to neglect self-management due to a lack of motivation, information, and knowledge; physical limitations; psychological and social problems; as well as economic burdens. As a result, these patients are at increased risk of disease progression, fatal complications, and death, compared to patients who are actively involved in self-management [13]. Accordingly, engaging these patients in self-management through self-empowerment requires a more individualized and specialized approach.
Therefore, this study aimed to investigate the effect of an empowerment program in patients with poor self-management on their self-management abilities, self-efficacy, and Health Related QOL (HRQOL). This study is premised on the following hypothesis: the experimental group who undertakes the empowerment program will have higher self-management, self-efficacy, and HRQOL scores than the control group after a three-month intervention.
METHODS
1. Study Design
This study employed a quasi-experimental design using a pre- and post-test nonequivalent control group to examine the effects of the empowerment program in patients with CKD.
2. Setting and Samples
Participants were recruited from a general hospital located in a metropolitan area of South Korea. The inclusion criteria were as follows: 1) patients with stage 2~4 CKD, 2) middle-aged and elderly (≥40 years) patients, and 3) patients who understood the study procedure. Patients with a recent episode of ischemic heart disease, current malignancy, or any other physical and/or mental conditions that may have influenced their ability to participate in the study were excluded.
Participants were selected from patients who visited the outpatient clinic every three months. As a result of a short data collection period, the pool of participants unable to perform self-management in the experimental group was not large. Consequently, the experimental and the control groups were selected from patients with different patterns of self-management. That is to say, the experimental group was selected from patients who had difficulty with self-management, while the control group was selected from patients who had no problems with self-management and were waiting for renal outpatient treatment. The criteria for self-management difficulty were based on the professional opinion of the nephrology doctors. The physician first checked the patients who did not follow the treatment regimen for three months, confirming their noncompliance with treatment guidelines such as diet and exercise. After confirming that the patients satisfied the inclusion criteria, researchers explained the study and asked patients in both groups if they were willing to participate in the study. The patients were informed that they could withdraw from the study at any time, and their voluntary participation was confirmed by a signed agreement.
The number of participants was calculated using G* Power 3.1 software based on previous research results [9]. The effect size for the Analysis of Covariance (ANCOVA) test was calculated as 0.54, α 0.05, and power 0.80, and the results of 50 participants were calculated in total. A total of 58 patients were required for each group in anticipation of some dropping out. A total of 47 patients were assigned to the experimental group by nephrologists: three did not meet the inclusion criteria and 15 refused to participate. A total of 55 patients from the outpatient department were asked to participate in the control group: five did not meet the inclusion criteria and 21 did not consent to participate in the study. As a result, 29 patients were assigned to each group and the three-month intervention was performed. Two participants in the experimental group did not participate in all sessions of the intervention, and one from the experimental group and two from the control group did not participate in the post- test (Figure 1).
3. Ethical Considerations
This study protocol adhered to the Declaration of Helsinki, and all study procedures were reviewed and approved by the Institutional Review Board (IRB) at Ilsan Hospital in Gyunggi province, where the trial was conducted (IRB No: CR 2013-076).
4. Measurement / Instruments
The demographic and disease-related characteristics of the participants included age, gender, education, marital status, employment, underlying CKD, eGFR, and comorbidities at baseline. The eGFR was determined by the Modification of Diet in Renal Disease (MDRD) study equation considering gender, age, and serum creatinine level [14].
Self-management was measured using the “self-management instrument” for CKD developed by Lee and Kim [15]. This instrument comprises 23 items in the following five categories: 1) compliance with the treatment regimen and partnership (seven items), 2) dietary compliance (four items), 3) problem-solving (five items), 4) health behaviors (three items), and 5) pursuit of psychosocial well-being (three items). A 5-point Likert scale ranging from 0 (never) to 4 (always) is used. The total score ranges from 0~92 points, with higher scores indicating a higher level of self-management. The Cronbach's α coefficient of this tool was .85 in the present study.
A self-efficacy questionnaire was developed based on the aforementioned “self-management instrument”[15]. After constructing questions representing the five categories of self-management, the research team discussed and revised it to comprise five items for assessing the patients' beliefs in dealing with each self-management ability, including confidence regarding treatment compliance, dietary compliance, problem-solving, healthy behavior, and stress management. The instrument used in this study employs a 5-point Likert scale. The total score ranges from 0~20 points, with higher scores indicating a higher level of self-efficacy. The Cronbach's α coefficient of this tool was .76 in the present study.
HRQOL was assessed using the Short Form (SF)-36 version 2 questionnaire [16], which consists of 36 items divided into eight subscales. HRQOL scores are summed into a Physical Component Summary (PCS) and Mental Component Summary (MCS). In this study, both PCS and MCS were calculated using the Quality Metric Health OutcomesTM Scoring Software 4.5, with scores ranging from 0~100. Higher scores indicate better health-related QOL.
5. Data Collection
Data collection and intervention was performed from March to September 2014 at Ilsan Hospital in Gyunggi province, Korea. Baseline measurements were taken from the study outcomes-including self-management, self-efficacy, and HRQOL; measurements were taken again at the end of the three-month intervention period. The data were collected by research assistants who were blind to the group assignment. A small gift was given to each participant who completed the questionnaires as a token of appreciation.
6. Intervention
The theoretical framework of the empowerment program was based on the self-regulation model of disease prevention and management. The major principle of this model is that patients play the most important role in managing their disease. The core process is self-regulation, managing their disease by observing, judging, and reacting, continuously and reciprocally [17]. Health educators can enable individuals to build their observation skills by suggesting various means of self-monitoring, improve their ability to make judgments by establishing criteria for self-assessment, and develop their capacity to react appropriately by encouraging realistic evaluations of their self-efficacy and outcome expectation.
In this study, strategic interventions for disease management were conducted through empowerment programs, and the modified reaction was performed through the reciprocal self-regulation process (Figure 2). Different empowerment interventions have expected varying outcomes because empowerment differs according to intrapersonal, interactional, and behavioral components across people, contexts, and time [18]. This empowerment program emphasizes that active factors ultimately empower the patient to perform self-management by promoting management skills and enhancing their self-efficacy and problem-solving skills.
Interventions for the experimental group included an initial assessment, individualized goal-setting, health education, and support via small group sessions and individual phone counseling (Table 1). The initial assessment included a review of treatment progress, medication compliance, lifestyle and health behaviors, and a psychosocial evaluation through an interview. Individualized goals were set based on the initial assessment results. Small group sessions and phone counseling were each held four times in the three-month intervention periods. The small group discussion consisted of six groups of four-five people. The small group sessions were conducted for two hours at three-week intervals and led by three research nurses, as well as other health professionals such as a nephrologist and a dietitian. Group discussions based on patients' life experiences, as well as question and answer techniques, were used to make patients aware of their own coping strategies and problem-solving techniques, as well as those of others. Individual phone counseling followed within one week of each group session, according to a standardized counseling protocol. The counseling sessions were led by the same nurses who were in charge of each small group discussion, and intended to enhance self-efficacy, monitor patients' self-management, and address their problems. The control group participants received the usual care, including an evaluation of clinical indicators and recommendations for lifestyle modifications, as they usually did during a clinical visit.
After enrollment and baseline assessment, all participants were provided a self-help CKD management booklet developed specifically for this study. The booklet included general information on renal health, the management of complications, treatment regimens, and lifestyle modifications.
7. Data Analysis
All statistical analyses were performed using SPSS version 18.0 (IBM Corp., Somers, NY, USA). Descriptive statistics, an independent t-test, and χ2 test were used to compare the characteristics and outcome variables of the groups at the baseline. Since the result of the self-management score in the pretest was not homogenous, the ANCOVA test was used to analyze the differences between the experimental and control groups in terms of the extent of change in the study outcomes after controlling for baseline scores.
RESULTS
The mean age of the patients in the experimental group was 63.1±10.6 years (range: 41~79 years) and 67.3±10.2 years (range: 46~79 years) in the control group. The mean eGFR value was 43.7±13.0 mL/min/1.73m2 in the experimental group and 45.6±11.3 mL/min/1.73m2 in the control group. No differences were observed in the baseline participant characteristics between the two groups (Table 2). However, the self-management of the research outcomes was different between the two groups (t=−3.50, p=.001). Therefore, we analyzed the outcomes adjusted for the self-management scores (Table 3).
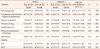
The hypothesis that self-management, self-efficacy, and quality of life scores would be higher in the experimental group than in the control group following a three-month intervention was supported. However, the hypothesis regarding the two categories of the self-management instrument was rejected. Based on the ANCOVA results, significant improvement was observed in the experimental group compared to the control group in terms of overall self-management (F=9.21, p<.004) and self-efficacy (F=5.81, p<.020). In the category of self-management, the experimental group showed improvement in the items of dietary compliance (F=8.07, p<.006), problem-solving (F=18.28, p<.001), and pursuit of psychosocial well-being (F=9.30, p<.004). However, no improvement was seen in compliance with treatment regimen and partnership (F=1.17, p<.284), and healthy behaviors (F=0.77, p<.384). In addition, the HRQOL improved significantly in the experimental group in comparison to the control group, as evidenced by improvements in the mean score on the PCS (F=5.94, p<.019) and MCS (F= 6.82, p<.013) (Table 3).
DISCUSSION
We hypothesized that this empowerment program would affect patients' self-management and self-efficacy, and that this would likely influence their QOL. Several studies suggest that the empowerment of CKD patients is associated with outcomes such as improvements in QOL [919] and enhancement of self-efficacy [9]. These outcomes are somehow related to the concept of self-efficacy. Self-efficacy, however, has been referred to in different ways, such as the goal of an empowerment-based intervention, indicator of empowerment, predisposing factor, and the acquisition of necessary skills for an empowerment process [20]. In this study, we have defined self-efficacy as the acquisition of necessary skills for an empowerment process. The ultimate goal of an empowerment program is improving the ability to actively participate in everyday self-management through the pursuit of self-efficacy according to outcome expectations.
In the current study, self-efficacy and three categories of self-management (dietary compliance, problem-solving, and pursuit of psychosocial well-being) improved. However, no improvement was seen in two categories: namely, compliance with treatment regimen and partnership, and healthy behaviors. The substantial improvements in patients' overall self-management skills observed in this study shows that intervention focusing on the practical development of problem-solving skills and enhancement of self-efficacy may have empowered the patients who have difficulty with self-management. These results support the results that problem-solving and self-management education had major clinical and behavioral outcomes in chronic patients [21]. The practical process of problem-solving was incorporated into this program to help patients identify effective solutions using personal, environmental, psychosocial, and knowledge based resources. During the group discussions, the participants obtained insight into effectively dealing with their problems through a problem-solving simulation using their own issues. They shared their feelings and experiences regarding their successful or unsuccessful ability to cope with their physical and emotional problems. The results of this study suggest that the use of peer mentors has a significant effect on the management of chronic patients [22].
Dietary compliance is the most difficult task for patients with stage 2~4 CKD. More specifically, patients who do not have good self-management struggle the most in following the diet regimen [23]. The dietary education provided during group sessions and telephone counseling helped patients meet personal goals and needs, and may have led to positive changes in dietary compliance.
Common barriers to self-management are chronic conditions accompanied by a negative psychosocial and emotional state [24]. In turn, this can affect a patient's ability to overcome the problems they encounter. As such, the improved pursuit of psychosocial well-being may be considered problem-solving [9] and may also result in more energy for better disease management.
There was no significant difference in treatment compliance and partnership between the two groups. The main focus of this category is on compliance with treatment regimens and the ability to communicate with healthcare providers. Therapeutic communication facilitates the partnership between the patient and healthcare provider and motivates the patient to engage in self-management [25]. In Korean culture, however, the relationship between the patient and healthcare provider is hierarchical and passive rather than professional and coordinative. Previous studies have shown that the passive role of the patient makes it difficult to achieve the goal of decision-sharing central to the cooperative process between physicians and chronic patients [26]. Despite the fact that participants received empowerment intervention for their own health management in this study, the patients' age and short intervention periods may have prevented a change in this category.
Although some areas of self-management showed no improvements, the increase in patients' self-efficacy has enormous value because these beliefs can have a significant impact on the cognition and mental state of patients, influencing their ability to overcome the problems they encounter. As such, improved mental state can be considered problem-solving [9] and it may afford greater energy for better disease management.
Overall QOL was found to improve in most patients with CKD after self-management interventions [27]. However, some studies have suggested that such an improvement was observed only in mental QOL and that physical QOL did not change significantly [28]. Although this study involved a three-month intervention, it is encouraging to note that both physical and mental QOL improved. This may be because the research team collaborated in various ways to achieve the patients' goals. However, it is unclear how long these improvements can be sustained. In other words, given the difficulty of maintaining self-management in patients with chronic diseases, healthcare providers and patients need to constantly invest attention and effort to maintain self-efficacy. For ongoing management, recent reports suggest that self-management behavior requires the involvement of a booster in chronic disease processes [29]. Moreover, since empowerment-centered intervention is facilitated by the cooperation of related medical professionals [30], it is important for healthcare professionals to collaborate and employ a multidisciplinary approach in working with patients with CKD. This program considered collaboration with patients and health professional as a key point to observe, judge, and change health-related behavior. However, this was not an easy process: the research team-including nurses, a doctor, and a dietician-was required to spend considerable time with patients in order to reach an agreement on problem identification and prioritization. They also worked together to identify the necessary strategies for the problem-solving, implementation, and evaluation of the action plan.
This study has some limitations. As this study sought to test an intervention for patients who have difficulty with self-management, convenience sampling was used instead of random assignment. Moreover, since there is no gold standard to determine the level of participation in self-management, the absolute level of poor self-management could not be determined. Consequently, we asked the patients' nephrologist to identify patients with self-management difficulties and then asked such patients if they were willing to participate in the study. While general characteristics and disease-related characteristics were homogeneous between the two groups in this study, we could not control confusion variables because we did not measure the degree of previous health education or experience that could affect intervention. The pretest self-management scores were lower in the experimental group than in the control group. Therefore, data were examined using an ANCOVA test by controlling for pretest scores. This study did not measure the physiological factors, recurrent signs and symptoms, or rehospitalization, among others, which could directly represent the progress of the disease.
This study is valuable in that it targeted a difficult-to-reach population with the clear purpose of enabling them to engage in better self-management. The significance of this study lies in its findings: self-efficacy and overall self-management improved in the experimental group after the three-month intervention, although the experimental group comprised patients with poor self-management while the control group comprised general patients with CKD.
These results indicate that this program was well received by the target population, and that it led to a short-term improvement in their self-management and HRQOL. This study also provides insights for health policymakers, health educators, healthcare providers, and researchers regarding the development and implementation of pre-dialysis education as well as CKD management. Moreover, the individual experiences and substantial and/or potential barriers to CKD management addressed by the participants during the present intervention were interesting. Further qualitative research on these aspects would be helpful in expanding the features of educational programs for this difficult-to-reach population, as well as other CKD populations.
CONCLUSION
Healthcare providers should make an effort to comprehensively assess the unmet needs of and barriers to self-management in patients and provide individually tailored empowerment based on their condition.
Our results show that the program tested in this study empowered patients with low self-management compliance. It also improved patients' HRQOL. Our results suggest that although it is burdensome for healthcare providers in terms of time and workload, intensive patient support is vital-particularly for such a difficult-to-reach population. Further research is warranted to develop innovative approaches to stabilize and maintain self-management in patients with chronic disease.




 XML Download
XML Download