

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Alpha-fetoprotein-producing gastric cancer (AFPGC) is a rare subtype of gastric cancer associated with a poor prognosis because it readily metastasizes to the liver and lymph nodes. Despite attempts to treat AFPGC using many types of therapies, the prognosis remains bleak. Here we report the case of a patient with AFPGC treated using multimodal therapy who survived for 5 years. In particular, we focus on the effectiveness of hepatic intra-arterial (HIA) chemotherapy combined with oral administration of sorafenib tosylate (sorafenib).
Case Report
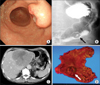
A 69-year-old man with upper abdominal pain was referred to our hospital in August 2006 by a local physician. Upper gastrointestinal endoscopy revealed a Borrmann type II-like tumor in the posterior wall of the lower part of the stomach (Fig. 1A). The biopsy specimen revealed well-differentiated adenocarcinoma, and immunohistological staining showed that tumor cells were positive for alpha-fetoprotein-producing (AFP). An upper gastrointestinal series radiography showed an elevated lesion with a central depression (Fig. 1B) in the lower part of the stomach. Laboratory examination revealed mildly elevated levels of aspartate aminotransferase (AST 67 IU/L), lactate dehydrogenase (834 IU/L), and alkaline phosphatase (565 IU/L). Serum level of carcinoembryonic antigen and CA19-9 was normal, but that of AFP was markedly increased (160,000 ng/ml).
Abdominal contrast-enhanced computed tomography (CECT) revealed a 14 cm long hypovascular tumor in the left lobe of the liver (Fig. 1C). On the basis of these findings, we diagnosed AFPGC with synchronous liver metastasis.
Our initial treatment plan was to perform a distal gastrectomy and an extended left lobectomy of the liver. However, another liver metastasis was found in the right lobe of the liver by the intraoperative sonography. We limited the surgery to distal gastrectomy with D2 lymph node dissection and Billroth I reconstruction in August 2006. The resected specimen was determined to be a 2.8 cm long Borrmann type II-like tumor (Fig. 1D).
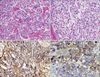
Histopathological examination of the gastric tumor revealed a well-differentiated adenocarcinoma with neoplastic growth of hepatocyte-like cells (Fig. 2A). The level of invasion was submucosal and 3 of 35 dissected lymph nodes were positive for metastasis. Intraoperative biopsy of the liver tumor showed features similar to those of the gastric tumor (Fig. 2B). Immunohistological staining showed that tumor cells in both the gastric tumor (Fig. 2C) and the biopsy specimen from the liver tumor (Fig. 2D) were positive for AFP.
After surgery, we placed a catheter into the proper hepatic artery for HIA. Chemotherapy using oral tegafur/gimeracil/oteracil potassium (TS-1, Taiho Co. Ltd., Tokyo, Japan) (120 mg/body/day from days 1 to 21)/HIA-cisplatin (CDDP) (30 mg/body/day on days 8 and 21, every 28 days) was started at day 15 after the surgery. After 4 courses, CECT revealed that the size of the metastatic tumor in the left lobe had decreased to 53.6% of the peak (Fig. 3A), and the small liver metastasis had disappeared. The serum AFP level had decreased to 2,910 ng/ml.
Six months after the surgery, the serum level of AFP began to increase, that is why we performed a left lobectomy. The resected specimen showed atrophic change in the left lobe and an odd-shaped soft liver tumor (Fig. 3B). On cut sections, the tumor was yellowish and highly denatured (Fig. 3C). Microscopic findings revealed degenerative changes and necrosis in almost all sections of the tumor. Viable cells were similar in structure to the microscopic findings of the primary gastric cancer. After liver resection, 9 courses of adjuvant oral TS-1/HIA-CDDP and oral TS-1/CPT-11 by drip infusion of vein (div) were administered.
Twenty-five months after the first surgery, we performed a partial lung resection because of new metastasis to the lung (Fig. 3D). Four months after partial lung resection, radiotherapy was performed to treat 2 new lung metastases. We obtained complete response transiently, but another new lung metastasis and para-aortic lymph node metastases appeared immediately. To treat these metastatic lesions, we performed chemotherapy sequentially as follows: 6 courses of paclitaxel (PTX) (div); 2 courses of 5'-Doxifluridine (DFUR) (oral)/Docetaxel (DOC) (div)/CDDP (div); 5 courses of DFUR (oral)/DOC (div); 8 courses of intravenous injection of 5-fluorouracil (5FU)/Adriamycin/Mitomycin-C (FAM); 2 courses of TS-1 (oral)/CPT-11 (div); and 6 courses of PTX (div) (Fig. 4).
In spite of these combination chemotherapies, metastatic lesions became difficult to control at 54 months after the first surgery, and the serum AFP level rose to 84,434 ng/ml. Liver metastases (Fig. 5A) and mediastinal lymph node metastasis enlarged gradually (Fig. 5B). The patient complained of respiratory distress resulting from bronchial oppression by enlarged lymph nodes. We could not use trastuzumab because immunohistochemical analysis revealed that human epidermal growth factor receptor type 2 was not expressed in either the primary lesion or the metastatic liver tumor. We proposed best supportive care, but the patient wanted to try a molecular-targeted drug. The administration of oral sorafenib tosylate (sorafenib) was begun at a dose of 800 mg/body/day using of a private import. After 2 months, his serum level of AFP dropped from 100,000 to 59,198 ng/ml. CECT revealed marked attenuation of vascularity at the liver metastasis, but a decrease in tumor size was not observed (Fig. 5C). The mediastinal lymph nodes shrunk in size by 16.2% (Fig. 5D). The patient's respiratory distress was completely alleviated, and stable disease was observed for a period of 4 months. The only adverse events observed were grade 1 hoarseness, increased AST, and hand-foot syndrome. The patient eventually died from cancer cachexia at 60 months after the first surgery.
Discussion
AFPGC is a rare tumor, accounting for only 1.3~15% of all gastric cancers.1 Previous reports suggest that the poor prognosis of AFPGC relative to non-AFPGC is because of its biological aggressiveness, as evidenced by its higher frequency for liver and lymph node metastasis.1-3 AFPGC with liver metastasis has a particularly dismal prognosis, regardless of whether it is synchronous or metachronous. Previous studies showed that the 5-year survival rate and median survival times were 0~3.8% and 9~11.4 months, respectively.1,4
On the other hand, several recent studies have demonstrated that AFPGC is highly chemosensitive compared with non-AFPGC. Kochi et al.5 reported the effectiveness of systemic 5FU/leucovorin/etoposide/CDDP (FLEP) combination therapy. After treating 10 patients with AFPGC and 47 with non-AFPGC using the FLEP regimen, they concluded that the AFPGC patients had a significantly better response rate and better disease-free and overall survival. Inoue et al.6 reported that 4 AFPGC patients with liver metastasis survived for 5 years through multimodal therapy and concluded the prognosis of AFPGC is not as poor as previously thought. These studies encourage us to not give up when treating AFPGC patients. However, to the best of our knowledge, only 10 cases have been reported in which the patient achieved 5-year survival when liver metastasis were present.6-8
In our case, metastasis was initially limited to the liver, so we selected HIA-CDDP combination chemotherapy with the objective of increasing the level of CDDP inside the liver tumor. In addition to the direct response against the large liver metastasis, we thought this drug combination might prevent further liver metastasis. Three AFPGC patients treated with HIA were previously reported to have survived over 5 years. Sakurai et al.9 administered oral tegafur/uracil (UFT)/HAI-FAM, and the patient survived for 6 years. The administration of HAI-CDDP/MMC by Kajikawa et al. resulted in the 6-year survival of the patient. Kobayashi et al. administered UFT/HIA-MMC orally, achieving an 11-year survival.7 Several reports suggest that even when long-term survival is not achieved, HIA-treatment might improve the prognosis over that of systemic chemotherapies.10,11 We think that a regimen containing HAI is worth trying if metastasis is limited to the liver.
A significant finding brought forth by this case is the effectiveness of sorafenib in treating metastatic AFPGC lesions. Sorafenib is a multi-kinase-targeting oral drug that inhibits intercellular signaling pathways and extracellular receptors, including vascular endothelial growth factor receptor and platelet-derived growth factor receptor.12 In patients with advanced hepatocellular carcinoma (HCC), randomized studies revealed that sorafenib prolonged the median survival time by nearly 3 months.12 Recently, Kim et al.13 showed the effectiveness of sorafenib in combination with CPT-11/CDDP systemic chemotherapy as a first line therapy for advanced gastric cancer. They reported the response rate was moderately high (62.5%, 10 of 16 patients), but the median overall survival was <1 year.
Several studies have reported that the hepatocyte growth factor (HGF)/c-Met pathway is activated in both AFPGC and HCC.14,15 Activated HGF/c-Met has been observed to enhance downstream signaling cascades such as the JAK/STAT3 and Raf/MEK/ERK pathways, resulting in cell proliferation.15 One study reported that sorafenib inhibits these pathways and suppresses the progression of HCC.12 Sorafenib has been speculated to inhibit the activity of the Raf/MEK/ERK and JAK/STAT3 pathways in AFPGC as in HCC. Using CECT, we found that the vascularity of the tumors decreased markedly during sorafenib treatment. We hypothesize that the inhibition of VERFR and PDGFR by sorafenib led to this observed decrease in tumor vascularity. This report is the first to suggest the possible use of sorafenib for treating AFPGC. Further studies and clinical trials are required to confirm the efficacy of sorafenib in the treatment of AFPGC.



 XML Download
XML Download