

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Periodontitis is a common, multifactorial, chronic inflammatory disease of tooth supporting structures that is usually treated by means of nonsurgical (cause-related) therapy in the first phase. In addition to mechanical therapy of periodontitis, there are numerous adjunctive procedures that can potentially be beneficial for tissue regeneration and adequate immune response. After the cause-related therapy is completed, patients are scheduled for a re-evaluation in order to employ necessary further treatment procedures, such as surgical procedures [1]. However, some approaches use different procedures that can facilitate beneficial tissue response that may reduce or eliminate the need for surgical procedures. One of these procedures is microcurrent electrical stimulation, which is being considered as an additional treatment following conventional nonsurgical therapy of chronic periodontitis.
Periodontal ligament tissue consists of collagen fibers and cells, and periodontal ligament fibroblasts differ from other connective tissue cells by being rich in alkaline phosphatase, an enzyme that plays a major role in phosphate metabolism, that is, the process of mineralization [2]. In vitro studies of fibroblasts have shown that these cells proliferate more quickly when stimulated by a magnetic field. Yoshimura combined guided tissue regeneration with electric stimulation on class III furcation involvement and noticed increased osteogenesis, concluding that electric stimulation is an appropriate modality in reconstructive therapy [3].
Microcurrent, measured in microamperes (µA), mimics the electricity at the level of cellular processes during the synthesis of adenosine triphosphate (ATP) and proteins. It is also known as biostimulation or bioelectricity. Cheng et al. [4] studied different intensities of electricity in the healing process, and its effect on three parameters: 1) production of ATP, 2) protein synthesis, and 3) membrane transport. ATP production was increased by 500% when 500 µA was used. However, it decreased between 1,000 to 5,000 µA, and finally dropped below detectable levels at the intensity of 5,000 µA. Furthermore, electricity has been used in medicine to stimulate tissue regeneration [5,6]. Nessler and Mass [7] reported that the mean (14C) proline and (14C) hydroxyproline activities were 91% and 255% greater, respectively, in the tendons of rabbits when stimulated in vitro with 7 µA.
Enhanced wound and bone healing has been observed after applying a low intensity direct current. Decubiti in the lower leg and sacral area were stimulated with current ranging from 200 to 800 µA, and it was found that the stimulated wounds healed 1.5 to 2.5 times faster than normally. The wounds also required less debridement, and healed with more resilient scars [8-10]. In the field of dental research, the impact of electricity on periodontal tissues was assessed on beagle dogs, using intraoral application of electrodes on the bone defects. Results showed that electrical stimulation has the potential to stimulate regeneration of connective tissue and bone [11,12].
When using a 3M Dental Electronic Anesthesia System 8670 (3M Dental Products Division, St. Paul, MN, USA), a successful alleviation of pain sensations after scaling and root planing was reported [13]. Extraoral transcutaneous electric nerve stimulation (TENS) was studied for treating trigeminal pain analgesia and dental pain prior to restorative or endodontic treatment [14-16]. Stimulation of salivation and xerostomia alleviation produces good results in 2/3 of patients undergoing TENS treatment (placing electrodes on the skin in the area of the parotid glands) [17], while the impact on the periodontal tissues and healing in the oral cavity has never been tested. The secretion of saliva can be stimulated with the application of an intraoral microcurrent device [18].
The aim of the present study was to evaluate microcurrent electrical neuromuscular stimulation (MENS) when used as an adjunctive treatment to conventional nonsurgical periodontal therapy.
MATERIALS AND METHODS
Patient selection
A parallel-group, randomized, controlled clinical trial was designed to test the efficacy of microcurrent electrical neuromuscular stimulation (MENS) as an adjunctive treatment to nonsurgical periodontal therapy. Twenty patients (11 females and 9 males; mean age, 45.5±7.9 years) were recruited from the patient pool of the Department of Periodontology, School of Dental Medicine in Zagreb. Criteria for inclusion in the study were 1) generalized moderate to severe chronic periodontitis, and 2) at least four remaining teeth. We followed the American Academy of Periodontology/Centers for Disease Control and Prevention definition for moderate periodontitis and used at least 2 interproximal sites with clinical attachment loss (CAL) ≥4 mm not on the same tooth or at least 2 sites with probing depth (PD) ≥5 mm not on the same tooth [19]. The exclusion criteria were long-term medication (more than 5 years), systemic antibiotic therapy within the last 6 months, pregnancy, and systemic diseases and disorders affecting wound healing. Sites with furcation involvement were also excluded. All subjects were given oral and written information concerning the study and gave their written consent prior to the clinical examination. The study was conducted in accordance with the ethical principles of the Helsinki Declaration and had been approved by the local ethics committee (No. 05-PA-26-55/06).
Treatment protocol
An outline of the present study treatments is presented in Fig. 1. The periodontal examination included the assessment of plaque index (PI), bleeding on probing (BoP), PD, and CAL on all teeth. All measurements were recorded by a single blinded calibrated examiner at six aspects per tooth (mesiobuccal, mid-buccal, disto-buccal, mesio-lingual, mid-lingual, and disto-lingual) using a standard periodontal probe (PCP 15, Hu-Friedy, Chicago, IL, USA). The cemento-enamel junction or restoration margin was used as the fixed reference point. The examiner did not treat the patients and was also blinded to the fact that the patients were part of this study. PD and CAL measurements were observed for the molar (PD-M, CAL-M) and other, non-molar teeth (PD-O, CAL-O), respectively.
Five patients, each showing 10 teeth (single and multirooted) with PD >6 mm on at least one aspect of each tooth, were used to calibrate the examiner. The examiner evaluated the patients on two separate occasions, 48 hours apart. Calibration was accepted if the measurements at baseline and at 48 hours were similar to the millimetre at >90% level.
After giving written informed consent, patients were randomly assigned to one of the two treatment groups. Randomization was performed using a random number generator (Excel, Microsoft Co., Redmond, WA, USA). The test group (G1) was treated with nonsurgical periodontal therapy followed by 5 MENS treatments, whereas the control group (G2) was treated by means of nonsurgical periodontal therapy alone. Instrumentation of all target sites using ultrasonic and hand instruments was performed until the operator felt that the root surfaces were adequately debrided and planed without any setting of time standards. Patients received detailed oral hygiene instructions following debridement. After completion of nonsurgical therapy, subjects in the test group (G1) received five MENS treatments using a microcurrent device, the µ-med Dental Master MSG 1200 (Horst Kieserling, Waltenhofen, Germany). Patients were provided with five treatments during the three weeks following the initial therapy (Fig. 2). According to the manufacturer's instructions, each MENS treatment comprised the application of 8 electrodes for a period of 20 minutes. Four electrodes that promote healing of the inflammatory areas (output A: 5 minutes+150 µA 32 Hz and 5 minutes±40 µA 0.5 Hz, two on each side of the patient's cheek) and four electrodes that stimulate the lymph drainage (output B: 5 minutes+80 µA 300 Hz and 5 minutes±40 µA 300 Hz, two on a chin area and two on a clavicle area) were placed using ultrasound gel (Fig. 3). Re-evaluation of all clinical parameters was performed six weeks after therapy.
Statistical analysis
Data analysis was performed with statistical software package SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). All analyses were performed on subject-level data. Primary clinical outcome variables were changes in CAL and PD. Normal distribution of the values was assessed with the Kolmogorov-Smirnov test. Because all data were normally distributed, values for PI, BoP, PD-M, PD-O, CAL-M, and CAL-O were analysed with a parametric t-test. Baseline and re-evaluation differences within both groups were analysed using a paired t-test. For the statistical evaluation of the re-evaluation differences between the groups, the t-test was used. A P-value<0.05 was considered statistically significant. A calculation of sample size revealed that with 10 subjects in each group, there was 85% power to detect, at a 0.05 level, a true difference of 1 mm in PD reduction between the test and control.
RESULTS
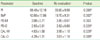
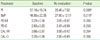
All 20 patients recruited for the study completed the trial, and the data were included in the statistical analysis. No complications or infections were observed throughout the study period. Results are summarized in Tables 1, 2, 3.
Plaque index
No differences were found between the test and control groups at baseline. In both groups, at the time of re-evaluation, the PI scores decreased significantly compared to baseline. The PI re-evaluation scores were lower in the control group, but not statistically significant compared to the test group.
Bleeding on probing
Baseline BoP values did not differ significantly in the test and control groups. Six weeks following nonsurgical periodontal therapy, a significant decrease in BoP values was recorded in both test and control groups. BoP re-evaluation scores were lower in the test group, but the difference was not statistically significant compared to the control.
Probing depth-molar teeth
Baseline PD-M values did not differ significantly in the test and control groups. Six weeks following nonsurgical periodontal therapy, a decrease in PD-M values was found in both groups, but it was not statistically significant. PD-M re-evaluation scores did not differ significantly between the groups.
Probing depth-non-molar teeth
Baseline PD-O values of the test and control groups did not differ significantly. Lower PD-O values were recorded in both groups six weeks following nonsurgical periodontal therapy, with a statistically significant decrease in the test group. Re-evaluation PD-O values did not differ significantly between the groups.
Clinical attachment level-molar teeth
No differences for CAL-M scores were found between the test and control group at baseline. CAL-M values were found to be lower in both groups at the time of re-evaluation, with a statistically significant decrease in the test group. A statistically significant difference in CAL-M re-evaluation values was recorded between the groups.
Clinical attachment level-non-molar teeth
No differences were found for CAL-O scores between the test and control groups at baseline. CAL-O values were lower in both groups at the time of re-evaluation, with a statistically significant decrease in the test group. Re-evaluation CAL-O values were significantly different between the groups.
DISCUSSION
This study was conducted due to lack of research on the effect of electrical neuromuscular stimulation on healing in the oral cavity. Use of microcurrents in medicine began during the 1970s, and many reports of its effectiveness have been published. Microcurrent therapy ranges from 1 to 600 µA and can rarely be sensed by the patient. Nevertheless, it takes effect on the cellular level, as documented by Cheng et al. [4], since a microcurrent increases the production of ATP and protein synthesis, while certain intervals stimulate human fibroblasts to secrete growth factors [20].
Transcutaneous and noninvasive stimulation was chosen in this study because of the performance of microcurrent devices that employ electrodes positioned on the skin in the area of inflammation, as opposed to intraoral devices. Invasive studies using intraoral application of electrodes to artificially induce periodontal pockets in the mandibles of dogs (6 weeks with stimulation for 14 hours per day) have shown excellent results. Pathohistological findings showed better results in the stimulated areas for each of the measured parameters (probing depth, length of the junctional epithelium, and bone and cement apposition) [12].
The results of this research are comparison of the early success of nonsurgical therapy and nonsurgical therapy supplemented with MENS. Re-evaluation was performed after 6 weeks since, according to Plemons and Eden [21], 4 to 6 weeks represents an adequate time for assessing the results of non-surgical periodontal therapy. Statistically significant differences in the baseline and re-evaluation plaque index indicate that the patients of this study mastered the control of plaque to a certain extent. Both groups showed a statistically significant reduction in inflammation, again proving the clinical importance of nonsurgical periodontal therapy. Based on many years of research in which patients were monitored after nonsurgical therapy, it is evident that when the periodontal status improves in the first 12 months, it can be maintained by the supportive periodontal therapy [22]. Probing depth was not significantly reduced after the nonsurgical therapy in the control group. However, since the success of nonsurgical therapy represents the key issue in the re-establishment of periodontal health [23], this result can be associated with a relatively small number of observed patients.
Statistically significant results of this study were evident for the clinical attachment level in the test group, while significant changes were not observed for the clinical attachment level in the control group. It is also important to note that the measured clinical benefit in the test group is in addition to the already marked benefits obtained by scaling and root planning alone in the control group. Thus, although the measured benefit - beyond scaling and root planing - was on a modest level, it should be considered clinically relevant. The results favor the hypothesis that microcurrent stimulates tissue healing and regeneration; this could be useful as an adjunct method following the standard nonsurgical treatment of chronic periodontitis, and as a part of supportive periodontal therapy. Nevertheless, a larger sample-size and longer follow-up is a prerequisite to confirm our findings. Based on the results of the present study, future research should have a follow-up of at least 6 to 12 months to additionally assess bone regeneration.
A number of indications for MENS are usually mentioned, but there are only a few studies on this subject in this field. Based on the principle of the device, some possible indications could be the adjunctive treatment of periodontitis and gingivitis, postextraction wound healing, acceleration of osseointegration and healing after implant placement, postoperative reduction of edema, and alleviation of the temporomandibular joint disorders.
In conclusion, although the present study was limited to a short-term period of 6 weeks, the results indicate that the adjunctive application of MENS is a suitable supporting method to conventional periodontal therapy for chronic periodontitis. However, further studies with a larger sample-size and longer follow-up are required to confirm the findings of the present study.




 XML Download
XML Download