

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ergotamine has been used widely for the treatment of migraine, even though triptan derivatives have been accepted as the most effective agents for the relief of acute migraine attacks.1 Ergotism is a sustained vasospasm induced by ergot medication, and is very rare, but has been observed in various situations, mainly as a result of ergotamine overuse,2 idiosyncratic hypersensitivity reaction with therapeutic doses,3 and during concomitant use of other kinds of medication.4 The sustained arterial spasm observed in ergotism causes vascular insufficiency in the extremities, which is characterized by pallor, coolness, numbness, and claudication if not treated promptly, the affected limb(s) may develop dry gangrene and, less commonly, suppurative gangrene and sepsis.5
To treat ergotism, it is mandatory to discontinue the ergotamine as well as other provocative factors, and then a therapeutic strategy should be established to control the withdrawal symptoms and migraine.1 In cases of acute ergot toxicity, various levels of success have been reported with other treatment options, including calcium channel blockers, oral prazosin hydrochloride, alpha adrenergic blockers, systemic vasodilator therapy with nitroprusside, prostacyclin, and prostaglandin E.6,7
Here we describe a patient with ergotism who presented with typical angiographic findings involving both the upper and lower extremities, and who recovered after treatment, as assessed with the aid of improved vascular imaging.
CASE REPORT
A 48-year-old man was hospitalized for acute pain and weakness in both upper extremities, which had begun 3 days previously. He had no prior history of type 2 diabetes mellitus, hypertension, dyslipidemia, or trauma. He was a current smoker consuming one pack daily for 30 years. Both of his upper extremities were pale and cold, with an absent radial pulse and markedly delayed capillary refill.
The patient had a long history of migraine without typical aura and had been taking 3 mg of ergotamine daily for more than 21 years, this had been prescribed at the local psychiatry clinic. During the week prior to his admission, he had increased his daily ergotamine intake as a result of severe headache related to psychological stress. Neurologic examination revealed abnormal sensory findings: paresthesia, numbness, and splitting (sharp) pain in both forearms and hands, which was aggravated by repeated shoulder or hand motion. Laboratory findings were unremarkable except for leukocytosis (18,400/µL).
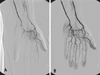
Emergency angiography of the upper and lower extremities revealed diffuse spasmodic narrowing along the proximal portions of both brachial arteries (Fig. 1A and B). At the distal portions of the right brachial artery, severe vasospasm and collateral formations were observed, and the ulnar and radial arteries were poorly visualized (Fig. 1C). Angiography of the lower extremities also revealed multifocal stenoses along the deep and superficial femoral arteries (Fig. 1D). The vascularity in the left hand was improved following infusion of prostaglandin E1 during the angiography (Fig. 2A and B), but the condition of the right upper extremity remained poor.
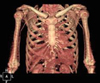
On the basis of the angiographic findings and the medication history, the patient was diagnosed as suffering from ergotism. During admission, smoking and all types of ergotamine and caffeine-containing drugs were discontinued. Intravenous nitroprusside was infused at a rate of 4 µg/kg/min, with itopride (50 mg) and propranolol (20 mg) also given twice daily. One day after the initiation of therapy, both radial pulses were palpable, and 2 days later the pain in the upper extremities had subsided, with minimal paresthesia. Nitroprusside was infused for 3 days, and then topiramate (50 mg) and flunarizine (10 mg) were started to treat withdrawal headache. Seven days after admission, the patient was discharged with clinical improvement. One month later, both brachial arteries appeared normal in a three-dimensional computed tomography angiogram (Fig. 3).
Three months later, the patient complained of irritability, insomnia, loss of appetite and libido, and psychomotor slowing that impaired his work. He was diagnosed with major depression by a psychiatrist, who prescribed paroxetine (25 mg daily). Over a period of 1 month, the dosage was increased to 32.5 mg/day and the depressive symptoms slowly improved.
DISCUSSION
Ergotism, the most notable toxic effect of ergotamine, causes vasospasm that can effect virtually any vessel, including the splanchnic circulation.1,5 In the present patient, angiography revealed thread-like narrowing with extensive collateral formation in the upper extremities, and segmental narrowing in the lower extremities. To the best of our knowledge, this is the first case of angiographically proven involvement of all four extremities, even though the pain and weakness were confined to the upper extremities.
The patient had been taking 3 mg of ergotamine daily for more than 21 years. Although most ergot toxicity is associated with excessive dosing, ergotism has been reported after extremely small doses or therapeutic doses administered over a long period of time.3,8 Furthermore, the patient might suffer from chronic migraine and therefore overuse his medication, as suggested by Silberstein.9 Recent mental stress and increased intake of ergotamine might have provoked the ergot intoxication in our patient. However, the acute vascular insufficiency resolved rapidly after vasodilator infusion without any definitive complication, and the headache was managed with recommended conventional prophylactic regimens.10
The patient described here suffered from psychiatric symptoms, and the diagnosis of depression was made after the treatment of acute ergotism. About 80% of chronic migraineurs are reported to have current psychiatry comorbidity.2 It is necessary to diagnose the psychiatric symptoms and add an antidepressant for appropriate management in chronic migraineurs and ergotism.
We present here a patient with ergotism, which was resolved by the discontinuation of ergotamine and infusion of a vasodilator, and which was diagnosed initially and followed up subsequently with vascular imaging.

 XML Download
XML Download