

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Over-concern with weight or height is increasing among Korean children.1,2 Currently, a tall and slender body configuration is considered to be ideal, and many schoolchildren seem to be dissatisfied with their weight and height.3-8 In western countries, many studies have been conducted on psychological issues in obese children,9-12 and most of them reported that overweight children are less adapted to environments,8 more depressive,9,10,13 and more anxious,10,14,15 and show lower self-esteem11,12,16 than their normal-weight peers. On the other hand, some studies reported contrary results.12,17 Weight issues have been more of a concern in recent years, but studies on psychopathology in short children are relatively rare. However, some studies reported that children with short stature suffer from low self-esteem, depression, social immaturity, behavioral problems, and academic difficulties,3-5,7,9-12,14,18-20 whereas other studies have failed to demonstrate the positive relationship between psychosocial or educational problems and short stature in school children.21,22 Although it is well documented that children with obesity or short statures tend to show more psychological problems than normal children, there have been no studies conducted in conjunction with underweight vs. obesity and short stature vs. tall stature together. Since children are growing, it is difficult to differentiate weight or height status. Height or weight standard deviation score (SDS) is the most exact validation marker of height or weight status by age and gender. This study was designed to assess the prevalence of body dissatisfaction, and the association between the weight and height status and a psychological problems among Korean elementary schoolchildren using SDS.
MATERIALS AND METHODS
Materials
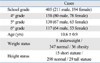
A total of 405 elementary school students (fourth to sixth-graders, aged 10-13 years, 211 boys and 194 girls), living in Seoul, Korea, were recruited from the community setting (Table 1). We excluded students who were diagnosed as having specific organic diseases, including a pathologically short stature or pathological obesity. The study was approved by the institutional review board of Sanggyepaik Hospital.
Measures
Height was measured to the nearest 0.1 cm on a harpendin stadiometer, and body weight was measured to the nearest 0.1 kg on a balanced scale by a trained nurse. Age and gender specific standard deviation scores (SDS) for the height and weight were calculated according to the physical growth reference data for Koreans.23 Height was categorized into three groups: short (< -2 SDS), normal (-2 SDS to 2 SDS), and tall (> 2 SDS), while weight was categorized into three groups: underweight (< -2 SDS), normal (-2 SDS to 2 SDS), and obesity (> 2 SDS).
The children were evaluated using the Korean version of the Child Behavior Checklist (K-CBCL).24 The CBCL crafted by Achenbach25,26 is a frequently-used questionnaire with 112 items, providing parent-reported data on problem behavior in children. A total problem behavior score was computed by summing the scores obtained for each item. The K-CBCL produces externalizing behavior problems, which are composed of attention problems and aggressive and delinquent behavior; internalizing behavior comprises withdrawal, depressed behavior, and somatic complaints. The social functioning scale includes socialization and academic functioning in the K-CBCL.
Body dissatisfaction was measured using the questionnaire developed by the authors, and this questionnaire included the degree of satisfaction about the subjects' height and weight. The degree of satisfaction was categorized into 3 groups: dissatisfied, fair, and satisfied. The subjects' economic status was categorized into 5 classes based on their parents' monthly income, according to the data from the Korean statistical office: high, middle high, middle, middle low, and low economic classes. The educational level of the parents was categorized into 5 groups: unschooled, elementary school, middle or high school, college/university, and postgraduate degrees. The height and weight of the subjects' parents and number of family member were also inquired.
Statistical analysis
All statistical analyses were performed using SAS software (version 9.1.3 SAS Institute, Cary, NC, USA). Comparisons of the means of the variables between the two groups were performed using a Wilcoxon rank sum test. Comparisons of the means of the variables among three groups (by weight or height status) were performed by the Kruscal Wallis test. A chi-square test was used to determine the percentage of dissatisfaction by gender or weight/height status. Pearson correlation analyses were utilized in order to assess relationship between total problem scores and other environment factors.
RESULTS
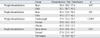
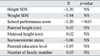
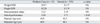
In this study, 34.4% of boys and 32.1% of girls showed dissatisfaction with their weight, whereas 26.2% of boys and 30.2% of girls showed dissatisfaction with their height (Table 2). The obese group showed higher weight dissatisfaction than the normal or underweight groups (p < 0.001). The short stature group showed higher dissatisfaction in their height than the normal group (p = 0.01) (Table 2). There was no significant difference in total CBCL problems score according to weight or height status (Fig. 1). The underweight and the obese groups had higher scores for social problems than normal weight group (p < 0.05 respectively) (Fig. 2). There were no significant differences in each CBCL problem score by height status. As a whole, the prevalence rate of CBCL total problems score in the clinical range was 3 percent (12/405). These children showed no differences in terms of weight or height, compared with normal students (Table 3). Among the factors related, only school performance was negatively correlated with the total problems score (p < 0.01) (Table 4).
DISCUSSION
There were three major findings from this study: 1) approximately one-third of elementary school students expressed dissatisfaction with their height or weight, 2) there was no significant difference in total CBCL problem scores according to weight or height status, and 3) the prevalence of problematic cases was 3 percent and the CBCL problems score was dependent on school performance, but not on weight or height status.
As expected, obese children showed significantly higher weight dissatisfaction than normal or underweight children. Prejudice and discrimination toward obese individuals persist despite nationwide increases in the prevalence of obesity in Korea.27 Negative attitudes and behaviors toward obese individuals are likely to be exacerbated by idealization of thinness that prevails in our society. Therefore, it is possible to consider that obesity leads children to have inferiority complexes about their outward appearance, to feel alienated, and to suffer from excessive stress.28 Obese adolescents are reported to be socially isolated and are likely to face difficulty when integrating themselves into the social network.29 Some studies demonstrated that overweight children had higher scores in social problems compared to normal children, whereas other studies showed no differences in anxious/depressed scale.11,30,31 Our findings are consistent with previous findings that obese children have high scores for social immaturity, but did not find significant differences in the anxious/depressed score. Since this is a population-based study which was confined to elementary school students, the prevalence of psychopathology may be lower than that in treatment-seeking clinical pubertal age samples. Interestingly, we found significantly higher social immaturity in underweight children than normal weight children. This implies that less attention has been paid to underweight children than to obese children, and they may also face serious psychological problems as well.
At present, Korean students are inclined to regard being tall as superior.19 In this study, 36.9% of short stature children are dissatisfied with their height. Social stereotypes for the height are established at an early age, and even young children ascribe positive attributes to tall children and negative attributes to short silhouettes.32 Although some researchers noted that short children have more emotional problems such as immaturity,33 anxious/depression, behavioral disorders, and social withdrawal than children with normal height,7,34 we did not find significant differences in terms of psychosocial problems in this study. This result might be ascribed to several factors. There is a possibility that children with short stature might have had less psychological problems even than medically-referred group because the present study was a population-based study. Another important factor is that we excluded pathologically short stature children because it is possible that idiopathic short stature has less psychological effects than pathologically (hormone deficiency or syndromatic) short stature. In addition, we confined our subjects to elementary schoolchildren, who were not seriously concerned about their short stature because of their future growth potential. Reijneveld et al.35 reported that the prevalence of CBCL problems score in the clinical range was 8.9% in the general childhood population, and Visser-van Balen et al.36 reported 7.8% prevalence in the medically referred idiopathic short stature adolescents. In this study, the overall prevalence of scores in the clinical range was only 3.0 percent (12/405). This low prevalence might be explained by different age distributions or ethnic backgrounds in the study population or by the fact that our study used CBCL data, which were reported by parents instead of children. The children whose CBCL total problems score were in problematic range showed no difference in terms of weight or height, compared with normal students. Among the factors related, only school performance was negatively correlated with the total problems score. This reflects the fact that fourth to sixth-grade children are more affected by their school performance scores than their height or weight status. Since the parental expectation of school performance in Korea is high, there is a possibility that children with low school performance may have increased psychological problems.
Our study has some limitations. First, our analysis is based on parent-reported CBCL data, which are less valid than children's self-reported data, and the questionnaire did not specify an accurate definition of the degree of body dissatisfaction. Second, the prevalence of problematic cases was too small to analyze the factors related. Third, pubertal adolescents could have different results. In spite of these limitations, our study is the first report which elucidated psychosocial problems in relation with weight and height status, using the validation marker of standard deviation score.
In conclusion, approximately one-third of elementary schoolchildren were dissatisfied with their height or weight. However, the total CBCL psychological problem scores were closely related with school performance, but not with height or weight status. Contrary to a general view, our study suggests that psychological problems in schoolchildren may be related more with school performance than body physique.


 XML Download
XML Download