

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Excessive internet game use despite dysfunction in daily life has become a global issue in the psychiatric field due to social problems in many countries (12). Based on this viewpoint, the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) has added Internet gaming disorder (IGD) to the emerging measures and models section (3). Among IGD patients, many have comorbid psychiatric problems (45). Major depressive disorder (MDD) and attention deficit hyperactivity disorder (ADHD) are 2 of the most common comorbidities (4).
The clinical usefulness of electroencephalography (EEG) in psychiatric fields has greatly increased with the emergence of quantitative analyzing methods such as quantitative EEG (QEEG), which can help identify characteristic EEG profiles associated with psychiatric disorders (6).
Spectral analysis of QEEG data can provide information regarding brain activity at different frequency bands, including delta (0.5–3.5 Hz), theta (3.5–7.5 Hz), alpha (7.5–12.5 Hz), and beta (12.5–35.0 Hz) from different electrodes placed on the scalp (6). Recently, there have been attempts to determine characteristic features of IGD using spectral analysis of QEEG (789). Participants with IGD had lower absolute power in the beta band and higher absolute power in the gamma band compared with healthy controls (78). Increased gamma absolute power was significantly associated with the severity of IGD as well as degree of impulsivity (7). Furthermore, additional studies have been conducted to identify the characteristics of spectral QEEG in patients with MDD (6101112). Although results from different studies remain controversial, elevated alpha band activity in QEEG, especially in the parietal and frontal or occipital regions, is a common feature often reported in MDD patients (101112).
Coherence analysis is a type of EEG connectivity measurement that estimates the neural connectivity between distinct brain electrodes in a given frequency band in the time domain (10). By analyzing coherence, valuable information can be obtained regarding underlying brain cortical coupling (13). Some researchers reported increased EEG connectivity in MDD patients, especially in the alpha band (1415), while others showed decreased connectivity (1617). However, studies on QEEG coherence analysis on IGD are limited.
This is the first investigation to directly compare QEEG features between MDD without comorbidity (MDD-only) and MDD comorbid with IGD (MDD+IGD). In this study, we aimed to determine the commonalities and discrepancies of functional brain connectivity of MDD-only and MDD+IGD participants using the coherence analysis of QEEG data. We hypothesized that patients with MDD+IGD would show decreased EEG coherence within the frontal executory area compared to MDD-only. In addition, we hypothesized that MDD+IGD patients would show greater reduction in EEG coherence between overall brain regions such as frontal-temporal, temporal-occipital, and parietal-occipital areas.
MATERIALS AND METHODS
Study participants
Fourteen male MDD+IGD patients (MDD+IGD group: mean age, 20.0 ± 5.9 years) and 15 male MDD-only patients (MDD-only group: mean age, 20.3 ± 5.5 years) agreed to participate in this study among patients who visited the Department of Psychiatry at Chung-Ang University Medical Center. For screening, all participants were evaluated through an interview regarding mood and anxiety, as well as online game playing patterns. All participants completed the Beck Depression Inventory (BDI) (18) and Young's Internet Addiction Scale (YIAS) (2). The inclusion criteria for the MDD+IGD group were; 1) male 13–30 years of age, 2) diagnosis of MDD based on the Structured Clinical Interview for DSM-5-Clinician Version (SCID-5-CV) (19), 3) satisfied the criteria for IGD based on Section III of DSM-5 (3), and 4) no history of psychotropic medication including antidepressants during the last month. The inclusion criteria for the MDD-only group were; 1) male 13–30 years of age, 2) diagnosis of MDD based on the SCID-5-CV (19), and 3) no history of psychotropic medication including antidepressants during the last month. The exclusion criterion for the MDD-only group was YIAS score > 50, indicating comorbid excessive game playing and gaming-related problems. The exclusion criteria for all 3 groups were 1) BDI score < 16, 2) past or current episodes of any other psychiatric diagnosis based on the SCID-5-CV (19) including ADHD, the most common comorbid with IGD in addition to MDD (4), 3) severe medical illness, 4) past or current substance use disorders, 5) current psychotropic medication use, or 6) a history of head trauma.
Measures
All participants were assessed using YIAS, BDI, and Beck Anxiety Inventory (BAI). Conners-Wells Adolescent Self-Report Scale (CASS) was administered to participants, and the Korean ADHD Rating Scale (K-ARS) was administered to one parent of each participant. EEG recordings were performed for all participants using a 21-channel EEG system.
Clinical symptom measures
YIAS consists of 20 self-evaluating questions rated by the interviewees on a 1 (rarely) to 5 (always) scale (2). A YIAS score above 50 is considered as problematic internet use (20). BDI is a commonly used 21-item inventory evaluating the severity of depressive symptoms in adolescents and adults (18). BAI is an evaluation tool for anxiety symptoms with somatic concerns and is composed of 21 self-report questions (21). Both tools consist of 21 self-report questions rated by the interviewees on a 0 (never) to 3 (very likely) scale. CASS, the adolescent form of the Conners Rating Scales-Revised (CRS-R) is used as an assessment scale for ADHD in adolescents 12–17 years of age (2223). The CRS-R is a multimodal assessment tool for youth behavioral problems and is comprised of forms for parents, teachers, and adolescents. In this study, we used the adolescent self-report form, CASS-Short Form, which contains 27 items rated by the interviewees on a 0 (never) to 3 (very likely) scale. The K-ARS was developed based on the Korean version of DuPaul's ADHD rating scale (24) and standardized by So et al. (25). It comprises forms for parents and teachers, and contains 18 items rated by interviewees on a 0 (never or rarely) to 3 (very often) scale. In this study, we used the K-ARS parent form.
EEG data acquisition
EEG recordings were performed for all participants by an EEG technician in an electromagnetically shielded room in the Chung-Ang University Hospital. The EEG activity was recorded while the participants' eyes were closed for 10 minutes. The participants sat in an upright position on a comfortable chair with neck rest and were asked to remain awake during the EEG recording. Data acquisition was performed using a 21-channel CMXL-P230 EEG system (Grass-Telefactor, West Warwick, RI, USA). EEG data were collected from 19 electrodes positioned on the scalp at Fp1, Fp2, F3, F4, F7, F8, Fz, C3, C4, Cz, T3, T4, T5, T6, P3, P4, Pz, O1, and O2, according to the International 10/20 system. Two additional electrodes were positioned on the ear lobe with A2 as the reference and A1 electrode as the ground. The electrode impedance was below 5 kΩ, and the EEG signal was band-pass filtered at 0.5 to 46.0 Hz. Data were sampled at a frequency of 256 Hz.
EEG preprocessing
Artifact-free 300-second periods were extracted from raw EEG data for analyses. Epochs of artifacts were eliminated from the analyses by visual inspection. EEG data analysis was performed using NeuroSpeed software (Alpha Trace Medical systems, Vienna, Austria). The inter-hemispheric coherences were computed to assess synchrony in the frequency ranges of alpha (7.5–12.5 Hz), and beta (12.5–35.0 Hz) between the following 4 pairs of homologous sites: Fp1–Fp2, F7–F8, T3–T4, and P3–P4. Additionally, intra-hemispheric coherence for alpha and beta frequency band was calculated between the following 8 electrode site pairs: F7–T3, F8–T4, C3–P3, C4–P4, T5–O1, T6–O2, P3–O1, and P4–O2. Because all of contrasts were prearranged, and there were no more of them than the degrees of freedom for effect, Bonferroni-type adjustment to alpha was not required (26). Epileptic activity and other abnormalities were excluded by a board-certified neurologist.
Statistical analysis
The demographic data including age, years of education, duration of illness, and clinical scale scores including YIAS, BDI, BAI, CASS, and K-ARS scores were analyzed by independent t-test. Differences in inter- and intra-hemispheric coherence values for the frequency bands between groups were analyzed using the independent t-test. Statistical significance was set at P < 0.05. All statistical analyses were performed using Stata/SE 12.0 software (Stata Corporation, College Station, TX, USA).
RESULTS
Demographic characteristics
No significant differences in age, years of education, and duration of illness were observed between MDD+IGD and MDD-only groups (Table 1). The mean YIAS score in the MDD+IGD group (mean ± standard deviation, 60.5 ± 20.9) was higher than that in the MDD-only group (21.1 ± 7.4; t = 6.67; P < 0.001). There were no significant differences in mean BDI score (MDD+IGD: 24.9 ± 5.8; MDD-only: 29.7 ± 8.8; t = −1.72; P = 0.096) or BAI score (MDD+IGD: 18.7 ± 6.3; MDD-only: 25.1 ± 11.3; t = −1.87; P = 0.072) between MDD+IGD and MDD-only groups. The CASS score in the MDD+IGD group (21.9 ± 4.2) was significantly higher than that in the MDD-only group (17.1 ± 5.7; t = 2.52; P = 0.018). The K-ARS score in the MDD+IGD group (14.1 ± 3.1) was also significantly higher than that in the MDD-only group (10.1 ± 2.7; t = 3.46; P = 0.002).
Table 1
Demographic characteristics of the study population
Data are presented as mean (standard deviation).
MDD+IGD = major depressive disorder comorbid with internet gaming disorder, MDD-only = major depressive disorder without comorbidity, YIAS = Young's Internet Addiction Scale, BDI = Beck Depression Inventory, BAI = Beck Anxiety Inventory, CASS = Conners-Wells Adolescent Self-Report Scale, ADHD = attention deficit hyperactivity disorder, K-ARS = Korean ADHD Rating Scale.
*P < 0.05, statistically significant.
Coherence analysis
Inter-hemispheric coherence
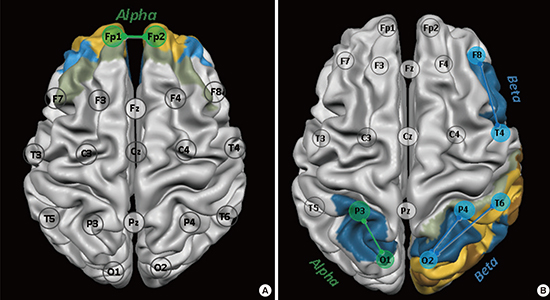
Inter-hemispheric coherence value for the alpha band between Fp1–Fp2 electrodes (t = −2.06; P = 0.049) was significantly lower in the MDD+IGD group than the MDD-only group (Table 2, Fig. 1A).
Table 2
Comparison of inter-hemispheric coherence values between MDD+IGD and MDD-only groups

| Variables | MDD+IGD | MDD-only | t | P value |
|---|---|---|---|---|
| Alpha | 0.049 | |||
| Fp1–Fp2 | 0.495 (0.260) | 0.651 (0.133) | −2.06 |
Fig. 1
Comparison of coherence between MDD+IGD and MDD-only groups. (A) Inter-hemispheric coherence. The value for the alpha band between Fp1–Fp2 electrodes was significantly lower in the MDD+IGD group than the MDD-only group. (B) Intra-hemispheric coherence. The value for the alpha band between P3–O1 electrodes and the beta band between F8–T4, T6–O2, and P4–O2 electrodes were higher in the MDD+IGD group than the MDD-only group.
MDD+IGD = major depressive disorder comorbid with internet gaming disorder, MDD-only = major depressive disorder without comorbidity.

Intra-hemispheric coherence
Intra-hemispheric coherence value for the alpha band between P3–O1 electrodes was higher in the MDD+IGD group than the MDD-only group (t = 2.12; P = 0.043). Intra-hemispheric coherence values for the beta band between F8–T4 (t = 2.06; P = 0.049), T6–O2 (t = 2.27; P = 0.032), and P4–O2 (t = 2.49; P = 0.019) electrodes were higher in the MDD+IGD group than the MDD-only group (Table 3, Fig. 1B).
Table 3
Comparison of intra-hemispheric coherence values between MDD+IGD and
DISCUSSION
In this study, we evaluated differences in QEEG features between MDD+IGD and MDD-only groups by analyzing inter-hemispheric and intra-hemispheric coherence. In summary, inter-hemispheric coherence value for the alpha band between right and left frontal regions was significantly lower in the MDD+IGD group than the MDD-only group. Increased intra-hemispheric coherence for the alpha band within the left parietal-occipital area was observed in the MDD+IGD group compared with the MDD-only group. The MDD+IGD group also showed increased intra-hemispheric coherence values for the beta band within the right frontal-temporal, temporal-occipital, and parietal-occipital areas compared with the MDD-only group.
So far, the results from several studies on coherence analysis in MDD remain controversial (1027), and no study has been conducted on coherence analysis in IGD. In the present study, inter-hemispheric coherence value for the alpha band between right and left frontal regions was significantly lower in the MDD+IGD group than the MDD-only group. These study results indicate greater attentive problems in MDD+IGD than MDD-only participants. In this study, the ADHD symptom scores among participants were significantly higher in the MDD-only group than the MDD+IGD group. Barry et al. (28) reported that children diagnosed with ADHD showed decreased inter-hemispheric coherence values for the alpha band in the frontal area in contrast to increased inter-hemispheric coherence values for delta and theta bands. We cautiously suggest that reduced inter-hemispheric coherence values for the alpha band in the frontal area in the MDD+IGD group indicated their attention problems at the subclinical level. In addition to MDD, ADHD is one of the most prevalent psychiatric disorders comorbid with IGD (429). Han et al. (30) suggested that ADHD children might use online gaming as a method of self-medication for improving attention and reducing distractibility by facilitating the cortico-striatal dopamine pathway. However, the effect is usually only temporary, and online gaming does not appear to provide IGD patients sufficient improvement of concentration in daily living. In summary, although not all participants in this study satisfied the diagnostic criteria for ADHD, there appears to be an association between decreased inter-hemispheric connectivity in the frontal region and vulnerability to attention problems in the MDD+IGD group.
The findings from intra-hemispheric coherence in this study can be explained both as a pre-morbid vulnerability for IGD and as a secondary change derived from repetitive online gaming (3132). First, we can explain increased intra-hemispheric coherence in various brain regions (frontal-temporal, temporal-occipital, and parietal-occipital) for alpha and beta frequency bands as a pre-existing vulnerability factor for IGD, that is, subclinical attention problems. Most previous studies conducting coherence analysis on ADHD reported increased coherence, mainly in the theta and beta bands (3334). Although none of the participants in this study satisfied the diagnostic criteria of ADHD, greater attentive problems in the MDD+IGD group than the MDD-only group may be associated with differences in intra-hemispheric coherence values between the 2 groups.
Conversely, the findings from intra-hemispheric coherence can be explained as a secondary change derived from repetitive online gaming (3132). Due to a lack of studies performing EEG in IGD, we can only refer to previous structural and functional magnetic resonance imaging (MRI) studies. In this study, increased intra-hemispheric coherence in the beta band within the frontotemporal area was observed in the MDD+IGD group compared with the MDD-only group. In their study using diffusion tensor imaging (DTI), Jeong et al. (32) showed increased white matter integrity measured using fractional anisotropy (FA) within the frontotemporal regions, which might be secondary to continuous online gaming. In a DTI study on healthy game users, Dong et al. (31) reported that severity of IGD was positively associated with FA values in the posterior cingulate and thalamus. Due to its important role in reward and sensory systems (35), the thalamus appears to be activated during game playing. Additionally, online gaming enhances the functions of brain regions associated with working memory and sensory-motor coordination including the frontal cortex (3637). Taken together, excessive activation of the frontal cortex and thalamus due to repetitive online gaming may be associated with increased intra-hemispheric coherence within the fronto-temporal area in participants with MDD+IGD.
In the present study, the MDD+IGD group also showed increased intra-hemispheric coherence in the beta band within the right parietal-occipital and temporal-occipital areas compared with the MDD-only group. The temporo-parieto-occipital junction, a complex brain circuit, is involved in diverse high-level neurocognitive functions such as language, self-processing, face and object recognition, symbol processing, and visuospatial working memory (38). Jeong et al. (32) reported increased FA values within the right inferior front-occipital fasciculus in IGD, which reflects visual motor information processing during online gaming. The authors also suggested that right-sided change appears to be augmented with online gaming and may be associated with the continuous burden of visuospatial working memory during gaming. In summary, neural connectivity between the right parietal-occipital and temporal-occipital regions may be increased by excessive online gaming in patients with MDD+IGD.
This study had several limitations. First, the number of study participants was relatively small to obtain universality of our results. Second, due to the cross-sectional study design, whether altered connectivity in MDD+IGD participants compared with MDD-only participants is a state marker that will improve after adequate treatment or a persistent trait marker of IGD is uncertain. Third, scalp EEG is an indirect measurement of brain activity and may infer brain activity overlying the various cortical regions. However, strong evidence shows a close correlation between signals from each EEG electrode and actual neural activity (3940).
In conclusion, there appears to be an association between decreased inter-hemispheric connectivity in the frontal region and vulnerability to attention problems in the MDD+IGD group. In addition, increased intra-hemisphere connectivity in the fronto-temporo-parieto-occipital areas may result from excessive online gaming. Further longitudinal studies are needed to explore whether the differences in QEEG findings are a state marker or a persistent trait marker of IGD. For example, if it is a trait marker, treatment for attentional problems for patients with MDD comorbid with IGD can be administered; if it is a state marker, gaming could be used as a training tool for enhancing neural connectivity of the temporo-parieto-occipital junction.
 XML Download
XML Download