

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
From the perspective of human history, lead is one of the ancient metals, extracted from ore and used as early as 6,000 years ago in Asia Minor. Lead was also used by the Egyptians in the arts and crafts around 3500 B.C. Some of the toxic effects of lead were probably known to both Greeks and the Romans. Hippocrates (circa 370 B.C.) describes a severe attack of abdominal pain (possibly lead colic) in a man who extracted metals, while Nicander, in the second century B.C., noted an association between exposure to lead and symptoms such as pallor, constipation, colic and paralysis (1). Lead serves no useful biologic function in humans, and lead exposure can result in acute or chronic adverse effects in multiple organ systems (2). The presence of lead in the environment has decreased since the 1970s when the US government enacted regulations banning the use of lead in gasoline, paint, and the soldering of cans (34). The blood lead levels in Korean lead workers and general population decreased and were similar to those in the US (56).
Republic of Korea (ROK) has a national ban on the possession of firearms. Therefore, it is impossible for a civilian to access firearms and ammunition, with the exception of licensed hunters and recreational shooters. However, because ROK remains under an armistice, it regularly consumes large quantities of ammunitions, with most of these ammunitions being used for training purposes. ROK has also recently begun a transition from outdoor firing ranges at military bases to indoor firing ranges, due to civilian complaints regarding noise. However, indoor firing ranges with poor ventilation systems increase the risk of exposure to shooting by-products (e.g., heavy metals), compared to outdoor firing ranges. Therefore, the present study aimed to investigate the risk of lead exposure (due to the firing of live ammunitions) among indoor firing range workers, and to determine the factors that were related to this risk.
MATERIALS AND METHODS
Subjects
The present study included a special health examination regarding lead exposure (April 2 to April 15, 2014) among 120 subjects, who included current workers at the indoor firing ranges of the Republic of Korea Air Force (ROKAF) and Navy, as well as professional military shooters belong to Armed Forces Athletic Corps. An occupational and environmental medicine specialist conducted individual interviews using a structured questionnaire regarding the subject’s occupational history. This questionnaire was followed by various anthropometric measurements, which included blood pressure readings. Diagnostic tests were also performed to evaluate the subject’s whole blood lead level (BLL), zinc protoporphyrin, blood urea nitrogen, creatinine, liver function, complete blood count, differential blood count, reticulocyte count, lipid profile, and urinalysis. An additional peripheral blood smear was performed for individuals who had a BLL of ≥ 10 µg/dL. Workplace environmental monitoring was also conducted at all firing ranges, with 3 site samples and 3 personnel samples from each firing range. The site samples were collected in the waiting rooms, firing points, and beaten zones of the firing ranges. The personnel samples were collected from the subject’s breathing zone. The sampling pump (Gilian, GilAir 5, Sensidyne Inc, USA) flow rates were calibrated before and after sampling using an automated bubble flow meter.
Job categories
The 120 subjects were classified according to their job type (shooting range supervisor, shooting range manager, and professional shooter) and rank (enlisted soldier, non-commissioned officer and commissioned officer). Shooting range supervisors only visited the firing ranges during shooting training to perform their duties (i.e., supervising the shooting process and training). Shooting range managers were stationed at the firing ranges and performed the overall management of the firing ranges. Their duties included organizing, cleaning up, and handling ammunitions waste after shooting training. Professional shooters were members of the ROK Armed Forces Athletic Corps, and this group included the shooters and the related staff members. Enlisted soldiers were fulfilling their mandatory military service duties in compliance with the Conscription Law; the duration of active duty military service is currently 21 months in the Army and Marine Corps, 23 months in the Navy, and 24 months in the Air Force. Commissioned officers were military officers with a rank of second lieutenant or higher, who were responsible for the command or operations of a corps or unit. Non-commissioned officers ranked between enlisted soldiers and commissioned officers, and assisted with the commissioned officer’s command and operations work.
Blood lead analysis
The BLL analysis was performed in a Republic of Korea Air Force research center (the Aerospace Medical Research Center), and the results were verified by an independent civilian analysis agency (Seoul Clinical Laboratories & Seoul Medical Science Institute). Because there were no significant differences in the analysis values (paired t test, P value > 0.1), the present study used the analysis values from the Aerospace Medical Research Center. The analysis method used in the Aerospace Medical Research Center was as follows. 0.1 mL of the whole blood was diluted with 1.8 mL 1%-triton X-100 and diluted solution was analyzed for BLL using graphite furnace atomic absorption spectrometry (NovAA 400p, Analytikjena, Germany). The standard addition method was used to prepare the standard curve. In an effort to verify validity and reliability of the analysis, the external quality control was carried out by the Korea Occupational Safety and Health Agency while the internal quality control was performed with standard reference material.
Statistical analyses
The χ2 test and Fisher’s exact test were used to compare the subjects’ general characteristics, and analysis of variance (ANOVA), the Kruskal-Wallis test, and Student’s t test were used to evaluate differences in age and BLL according to job type and rank. Because BLL exhibited a right skewed distribution, the data were subjected to a natural log transformation, its normality was verified, and the statistical analysis was performed. The standard for elevated BLL among adults is 10 µg/dL, as determined by the Adult Blood Lead Epidemiology & Surveillance from the National Institute for Occupational Safety and Health (NIOSH) (7). Therefore, odds ratio and 95% confidence interval were calculated using a multiple logistic regression analysis, with a BLL of ≥ 10 µg/dL as the dependent variable. The SPSS version 15.0 (SPSS Inc, Chicago, IL, USA) was used for data analysis. Statistical significance was defined as P value < 0.05.
Ethics statement
The subjects’ medical records were obtained by referencing the military medical information system and this study protocol was approved in advance by the institutional review boards of Medical Division of Headquarters, Republic of Korea Air Force (ROKAF-ASMC-2014-IRB-006). In addition, each subject provided written, informed consent before participating.
RESULTS
The mean subject age was 29.5 years, and the 120 subjects included 111 men (92.5%), 55 smokers (45.8%), and 74 alcohol drinkers (61.7%). The distribution according to rank was 32 enlisted soldiers (26.7%), 56 non-commissioned officers (46.7%), and 32 commissioned officers (26.7%) (Table 1). The sites that exceeded the permissible exposure limit (an 8-h weighted average of 0.05 mg/m3) were beaten zones (10/10; 100%), firing points (9/17; 53%), and waiting rooms (3/4; 75%). The ranks that exceeded the permissible exposure limit were shooting range managers (5/9; 56%), shooting range supervisors (3/5; 60%), and shooters (4/15; 27%). These results confirmed that the entire indoor firing range was exposed to airborne lead (Fig. 1).
Table 1
The subjects’ general characteristics
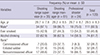
Fig. 1
Workplace environmental monitoring results from indoor firing ranges. TWA, time weighted average. *Results are presented as the mean (range). †Results are presented as (number of standard excess sites)/(number of monitoring sites) (%). The Occupational Safety and Health Administration (OSHA) standard for lead exposure is 0.05 mg/m3 of air, averaged over an 8 hours period.

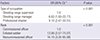
The BLL values were also analyzed according to job type and rank. The mean BLL among all subjects was 11.3 ± 9.4 µg/dL. The mean BLLs among the shooting range supervisors, professional shooters, and shooting range managers were 6.4 ± 3.1 µg/dL, 14.0 ± 8.3 µg/dL, and 13.8 ± 11.1 µg/dL, respectively (Table 2). The BLL was higher among professional shooters and shooting range managers, compared to that among shooting range supervisors; these differences were statistically significant. In all three groups, the BLL was highest among non-commissioned officers and lowest among commissioned officers (Fig. 2). Compared to shooting range supervisors, professional shooters and shooting range managers exhibited odds ratios of 9.10 and 6.62, respectively, for their BLL being ≥10 µg/dL; these differences were statistically significant. Compared to commissioned officers, noncommissioned officers and enlisted soldiers exhibited odds ratios of 16.10 and 13.90, respectively; these differences were statistically significant (Table 3).
Table 2
Distribution of blood lead levels according to job type and rank
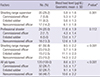
Fig. 2
Distribution of blood lead levels according to job type and rank. CO, commissioned officer; ES, enlisted soldier; NO, non-commissioned officer. *Comparison by analysis of variance. †Results are presented as the arithmetic mean ± standard deviation (range).

Table 3
Odds ratios and 95% confidence intervals for elevated blood lead levels (≥ 10 µg/dL)
To avoid additional blood exposure, subjects with a BLL of ≥ 10 µg/dL were immediately banned from the firing ranges, and follow-up monitoring of their BLL was performed 2 months later. At that time, their arithmetic mean BLL value exhibited a statistically significant decrease, from 16.61 ± 10.43 µg/dL (April 2014) to 9.78 ± 6.48 µg/dL (June 2014, P < 0.001).
DISCUSSION
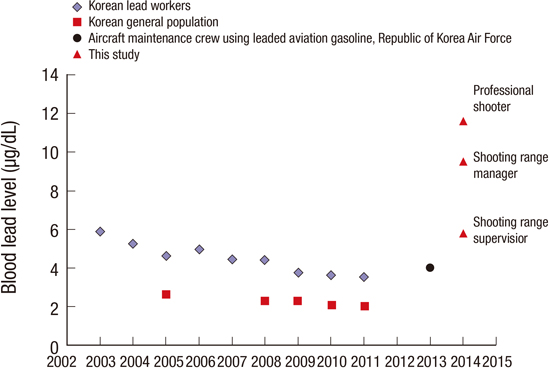
Because lead is very harmful to the body, having a lower BLL is preferable, and a BLL of ≥ 10 µg/dL is known to cause various adverse effects (89). Therefore, the BLLs that were observed in the present study are very alarming, as the mean BLL among all subjects was 11.3 ± 9.4 µg/dL (range: 2.0–64.0 µg/dL). Furthermore, the BLLs among professional shooters and shooting range managers were also extremely high (14.0 ± 8.3 µg/dL and 13.8 ± 11.1 µg/dL, respectively). These mean BLLs are much higher than the mean values from normal Korean adults or Korean lead workers (51011), and are also higher than those of ROKAF mechanics who work with leaded aviation gasoline (12) The geometric mean blood lead concentration in Korean adults was 1.99 μg/dL (95% CI, 1.94–2.05) from the 2011 fifth Korea National Health and Nutrition Examination Survey (Fig. 3) (1314).
Fig. 3
Geometric means of blood lead levels from Korean lead workers, general population and this study’s subjects.

In the present study, there were no significant differences in BLL according to age, smoking status, and tenure. This finding confirms the fact that the accumulation of lead was more closely associated with job type and rank, rather than tenure. Furthermore, this finding indicates that the accumulation of lead was closely associated with the subject’s specific duties. Therefore, the lead exposure inside firing ranges is likely related to the cleaning, handling of ammunition waste, and formation of air swirls (due to improper ventilation systems). Although poikilocytosis was observed in 4 subjects via their peripheral blood smears, we did not observe any hematological disorders (e.g., anemia), urological disorders, or neurological disorders. The absence of these disorders is likely related to the relatively short-term chronic exposure, as the indoor firing ranges were only recently implemented, as well as the nature of Korean military service, which requires a transfer in work location every 1–2 years.
The Occupational Safety and Health Administration’s occupational exposure limit for BLL is 40 µg/dL (15). In the present study, 1 (0.8%) non-commissioned officer who was working as a shooting range manager had a BLL of 64 µg/dL. Although other tests (e.g., nerve conduction velocity and electromyography) were performed for this subject, no other abnormal findings were observed. Furthermore, chelation treatment with CaNa2-ethylenediaminetetraacetic acid was completed without any adverse effects, and the subject’s BLL had reduced to 9.7 µg/dL after 3 months.
The present study evaluated personnel from the ROK Navy, ROKAF, and Armed Forces Athletic Corps, and excluded personnel from the ROK Armed Forces. The reason for the exclusion of ROK Armed Forces personnel was that this branch has a very low rate of transition from outdoor firing ranges to indoor firing ranges. This low transition rate may be affected by the related economic costs (due to this branch’s large size), and by fewer noise complaints (Armed Forces firing ranges are relatively far from residential areas). In contrast, the ROKAF and Navy are smaller than the Armed Forces, and are typically located near residential areas, which may have motivated the relatively high rates of transition to indoor firing ranges. Interestingly, our findings indicate that the large capital expenditure to build and improve indoor firing ranges actually adversely affected the health of military personnel. These findings may reflect the fact that an aesthetically pleasing and comfortable new facility is not always a healthy environment.
In ROK, occupational lead poisoning is uncommon, because lead exposure had been rapidly declining, due to improvements in occupational and environmental management (1617). Between 2000 and 2010, only 5 cases exhibited a BLL of > 40 µg/dL due to occupational causes, which indicates that the classical occupational lead poisoning has been well managed (181920). However, our findings indicate that the introduction of a new occupational environment may increase the risk of lead poisoning. For example, the risk of lead poisoning among indoor firing range workers has already been reported in countries with advanced shooting cultures and well-managed risk exposure (21222324). However, Korean experience in constructing indoor firing ranges is insufficient, which may be due to the restricted supply of firearms and the absence of firing range regulations. Therefore, when constructing indoor firing ranges, it is essential to employ a specialist to design and assess the ventilation system. Furthermore, safety guidelines regarding the handling of ammunition waste should be mandatory, and regulations regarding these issues should be implemented. Moreover, workplace environmental monitoring and special health examinations for firing range workers should be mandatory. Finally, status surveys and the management of lead exposure among professional shooters, instructors, and firing range managers should be performed by various agencies, such as the Korean Ministry of Culture, Sports, and Tourism and Korea Shooting Federation. For example, the current regulations for civilian recreational firing ranges lack clauses related to heavy metal exposure limits, and these issues must be considered in the future.
Based on the findings of this study, the ROK Ministry of Defense temporarily closed all indoor firing ranges and transferred anyone with a BLL of ≥ 10 µg/dL to units or divisions without exposure to lead. The indoor firing ranges are scheduled to reopen after improvements have been made to the ventilation system and environmental assessments have been performed. Moreover, the Ministry of Defense has also enacted safety and health management guidelines for indoor firing ranges. Therefore, before the transition from outdoor to indoor firing ranges (as in ROK), or before the establishment of new indoor firing ranges, it is essential that the facilities be constructed in a way that minimizes the lead exposure of the range’s workers and users.
 XML Download
XML Download