

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Yong Jae Lee, Jin Soo Suh, Jun Young Choi
Abstract
An osteochondral fracture is considered to be an injury involving the cartilage and subchondral bone. Acute traumatic osteochondral fractures can be related to joint instability because abnormal joint motion causes shearing and rotatory stress. Acute osteochondral fractures are frequently missed or misdiagnosed as a pure soft tissue injury. Thus, surgeons' proactive attention is highly required as articular cartilage has limited potential for self-repair and these lesions may develop osteoarthritis. In order to minimize the progression of post-traumatic osteoarthritis, it is important to properly identify and treat osteochondral fractures. Yet, little is known about the operative management of acute osteochondral fractures of the talus. We report here on a case of a middle-aged male with acute osteochondral fractures of the bilateral lateral talar dome. We applied different operative methods on each side with regard to fragment size and stability. A favorable clinical outcome was obtained at 18 months follow-up.
Figures and Tables
Figure 1
Right ankle anteroposterior (A), mortise (B) radiographs show a displaced osteochondral fracture of lateral talar gutter (arrows). (C) Fracture location is not certain on the lateral radiograph. Left ankle radiographs (D, anteroposterior; E, mortise) show no significant findings around talar gutter, while the lateral radiograph (F) shows small fracture fragment (arrow) from anterior tibial plafond.

Figure 2
Preoperative computed tomography shows a detailed nature of right (A, coronal; B, sagittal) and left (C, coronal; D, sagittal) talar gutter osteochondral fractures (arrows).

Figure 3
(A, B) Guide wire was passed through fracture fragment and talar body. (C) Then, bio-absorbable pin (Bioretec Ltd.) was fixed.

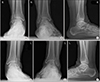
Figure 4
Immediate postoperative radiographs shows irregularity of lateral talar articular surface on the right side (A, anteroposterior; B, mortise; C, lateral) and absence of bony fragment on the left side (D, anteroposterior; E, mortise; F, lateral).
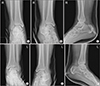
Figure 5
On the right ankle anteroposterior (A) and mortise (B) radiographs at postoperative 6 months, union of the fracture fragment was still processing with radiolucent lesion of the medial talar dome. (C, D) At 12 months postoperatively, suspicious osteochondral lesion of the medial talar dome became clearer.

References
1. Murawski CD, Kennedy JG. Operative treatment of osteochondral lesions of the talus. J Bone Joint Surg Am. 2013; 95:1045–1054. DOI: 10.2106/JBJS.L.00773.

2. Amendola A, Panarella L. Osteochondral lesions: medial versus lateral, persistent pain, cartilage restoration options and indications. Foot Ankle Clin. 2009; 14:215–227. DOI: 10.1016/j.fcl.2009.03.004.
3. Giannini S, Vannini F. Operative treatment of osteochondral lesions of the talar dome: current concepts review. Foot Ankle Int. 2004; 25:168–175. DOI: 10.1177/107110070402500311.
4. Rungprai C, Tennant JN, Gentry RD, Phisitkul P. Management of osteochondral lesions of the talar dome. Open Orthop J. 2017; 11:743–761. DOI: 10.2174/1874325001711010743.
5. Choi JY, Kim JH, Ko HT, Suh JS. Single oblique posterolateral approach for open reduction and internal fixation of posterior malleolar fractures with an associated lateral malleolar fracture. J Foot Ankle Surg. 2015; 54:559–564. DOI: 10.1053/j.jfas.2014.09.043.
6. Hermanson E, Ferkel RD. Bilateral osteochondral lesions of the talus. Foot Ankle Int. 2009; 30:723–727. DOI: 10.3113/FAI.2009.0723.
7. Verhagen RA, Struijs PA, Bossuyt PM, van Dijk CN. Systematic review of treatment strategies for osteochondral defects of the talar dome. Foot Ankle Clin. 2003; 8:233–242. DOI: 10.1016/s1083-7515(02)00064-5.
8. Hannon CP, Smyth NA, Murawski CD, Savage-Elliott I, Deyer TW, Calder JD, et al. Osteochondral lesions of the talus: aspects of current management. Bone Joint J. 2014; 96:164–171. DOI: 10.1302/0301-620X.96B2.31637.
9. Pedersen ME, DaCambra MP, Jibri Z, Dhillon S, Jen H, Jomha NM. Acute osteochondral fractures in the lower extremities - approach to identification and treatment. Open Orthop J. 2015; 9:463–474. DOI: 10.2174/1874325001509010463.
10. Di Cave E, Versari P, Sciarretta F, Luzon D, Marcellini L. Biphasic bioresorbable scaffold (TruFit Plug®) for the treatment of osteochondral lesions of talus: 6- to 8-year follow-up. Foot (Edinb). 2017; 33:48–52. DOI: 10.1016/j.foot.2017.05.005.
 XML Download
XML Download