

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tuberculosis (TB), caused by an infection of Mycobacterium tuberculosis, is the the most common cause of death from a single infectious agent among adults. Approximately one-third of the world's population (2 billion people) is thought to have latent M. tuberculosis, while an estimated 9 million people develop active disease from M. tuberculosis every year [1, 2]. The progression from latent to active TB commonly occurs in immunocompromised patients and is mainly related to dysfunctional cell-mediated immunity. Moreover, hematologic malignancies such as leukemia or lymphoma are thought to be risk factors for TB infection during cytotoxic chemotherapy [3]. Multiple myeloma (MM) is known to be associated with the immune abnormality hypogammaglobulinemia, which primarily affects humoral immunity. Recent studies suggested that the number of CD4+ T cells in MM patients is reduced at initial diagnosis and that the decline in CD4+ T-cell number was more severe in patients with refractory MM [4]. In addition, chemotherapeutic regimens for MM are known to induce immunosuppression.
Bortezomib is a proteasome inhibitor and one of the novel agents used in the treatment of MM. Bortezomib is known to induce apoptosis in rapidly proliferating and neoplastic cells, and a recent study showed that bortezomib prevents the activation of nuclear factor (NF)-kappa B. This leads to the inhibition of T-cell activation, including that of CD4+ T cells, which fulfill essential immune functions [5, 6]. Activation and proliferation of CD4+ T cells are crucial to the host's defense against TB infection [7]; thus, the suppression of T-cell immunity resulting from bortezomib-containing treatments potentially increases the risk of TB in MM patients [8]. The aim of our study was to investigate the incidence of TB in MM patients treated with a bortezomib-containing regimen.
MATERIALS AND METHODS
We retrospectively investigated the incidence of TB infection in 115 patients diagnosed with MM, who were treated with bortezomib-containing salvage chemotherapy between November 2004 and July 2010. Eighty-two patients received treatment with bortezomib (1.3 mg/m2 i.v. on days 1, 4, 8, and 11), cyclophosphamide (150 mg/m2 orally on days 1-4), thalidomide (50-100 mg/day orally every day), and dexamethasone (20 mg/m2 i.v. on days 1, 4, 8, and 11 every 3 weeks) (Vel-CTD), while 33 patients were given Vel-CD; Vel-CD is similar to Vel-CTD but does not contain thalidomide [9]. We retrospectively reviewed the medical records, including the clinical history, chest radiographs, and computed tomography (CT) scans prior to bortezomib-containing chemotherapy to assess evidence of previous TB infection and possible reactivation of the disease in the patients. TB was diagnosed on the basis of respiratory symptoms, chest CT scans, sputum M. tuberculosis culture, or acid-fast bacillus microscopy. Bronchoalveolar lavage or transbronchial biopsy was also performed for the diagnostic work-up in some patients suspected of having TB. We then investigated the clinical outcome, the control of myeloma tumor burden, and the cumulative dose of bortezomib in MM patients with a confirmed diagnosis of TB. We used the International Myeloma Working Group (IMWG) uniform response criteria to assess the treatment response in MM patients [10].
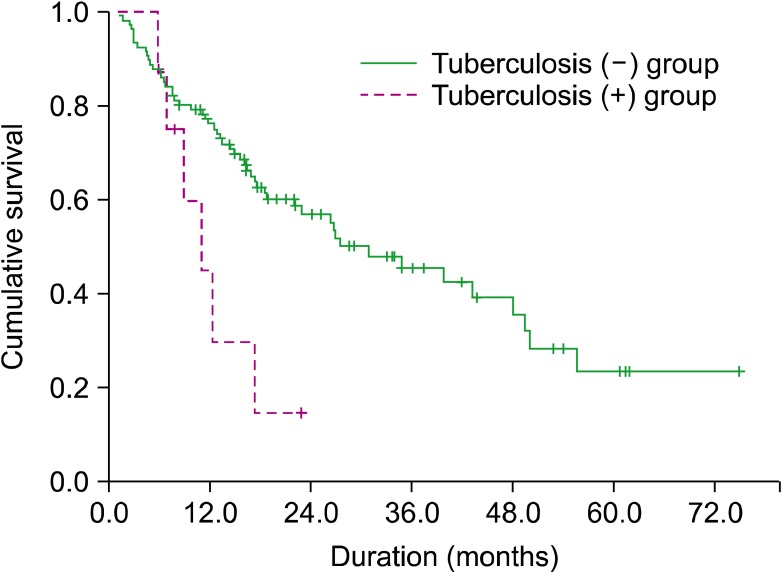
Categorical data and continuous variables were assessed using Fisher's exact and the Mann-Whitney U-tests, respectively. Overall survival (OS) was defined as the initiation of bortezomib-containing treatment to the date of the last follow-up or death. OS was analyzed using Kaplan-Meier survival curve estimates, and the differences between patients with (TB+) and without TB (TB-) was compared using stratified log-rank tests. A value of P <0.05 was considered statistically significant, and 95% confidence intervals were reported. All statistical analyses were performed using Statistical Package for the Social Sciences version 17.0 (SPSS, Chicago, IL, USA).
RESULTS
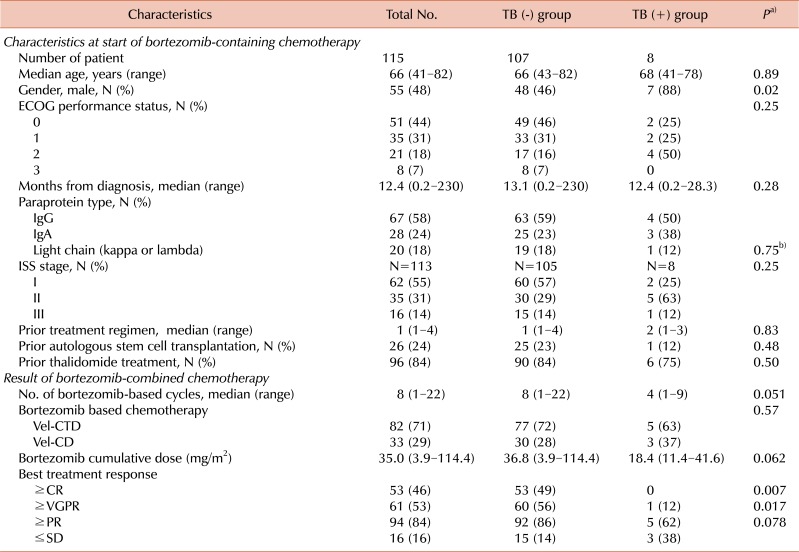
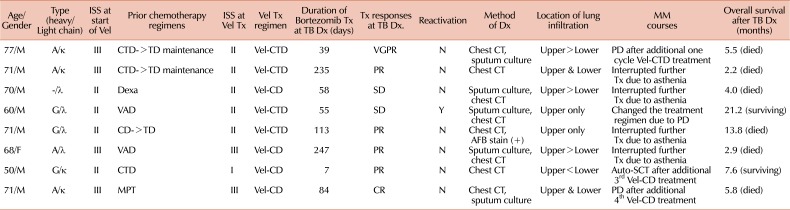
The median age of patients was 63 years (range, 39-82 years). All patients received chemotherapy prior to the initiation of a bortezomib-containing regimen, and the median number of prior regimens was 1 (range, 1-4). Patients received a median of 8 (range, 1-22) cycles of bortezomib-containing salvage chemotherapy. The median duration from diagnosis of MM to the bortezomib-containing chemotherapy was 12.4 months (range, 0.2-230 months), and 24% of patients previously received autologous stem cell transplantation (Table 1). Neither interferon-γ release assay (IGRAs) nor TB skin test was performed prior to the initiation of bortezomib-containing therapy. All patients were routinely evaluated for TB infection using simple chest radiography at the start of bortezomib-containing salvage chemotherapy, and 13 (11.3%) of the 115 patients underwent chest CT for the evaluation of associated lung abnormalities. One patient was diagnosed with active pulmonary TB prior to receiving bortezomib-containing chemotherapy, while 8 (7%) of 115 patients were diagnosed with TB infection during bortezomib-containing treatment (Table 1). The median duration from the start of bortezomib-containing treatment to the confirmed diagnosis was 58 days (range, 7-247 days). In all the patients who were diagnosed with TB during bortezomib-containing treatment, pulmonary infiltration was detected using chest CT. In 5 of these patients, TB infection was documented through sputum culture and in 1 patient, through sputum acid-fast bacillus microscopy. Two patients were diagnosed without bacteriologic confirmation because it was not possible to perform bronchoscopic evaluation due to grade 4 asthenia; nevertheless, the typical characteristics of TB on CT, such as bronchiectasis and centrilobular nodules with branching linear structures (tree-in-bud opacities) were observed. In addition, clinical symptoms were consistent with TB, and these patients did not have evidence of other non-TB diseases. Seven of the 115 patients showed signs of previous pulmonary granulomatous lesions at diagnosis of MM, but only 1 patient experienced reactivation of TB during bortezomib treatment. The baseline characteristics of patients enrolled in the study are reported in Table 1.
There was no statistical difference in age, performance status, paraprotein subtype, stage at the start of bortezomib-containing chemotherapy, and prior treatment between patients with (TB+) or without TB infection (TB-). The male gender was more frequently associated with TB+ (P =0.02). The median duration from the diagnosis of MM to the initiation of a bortezomib-containing regimen was 12.4 months in TB+ patients and 13.1 months in TB- patients (P =0.28). There was no difference according to the treated combination chemotherapies between groups (Table 1). All TB+ patients were treated with combination of isoniazid, ethambutol, rifampicin, and pyrazinamide (HERZ), and the intention was to treat all patients with this anti-TB regimen for a period of 6 months. However, all but 3 of the TB+ patients died of disease progression within the 6-month treatment period (Table 2), and only the surviving 3 completed the 6-month anti-TB regimen. None of the patients died of uncontrolled pulmonary TB infection; however, 4 patients had to discontinue bortezomib treatment because of grade 3 or 4 asthenia. TB+ patients received a median of 4 cycles of bortezomib-containing chemotherapy, and the cumulative dose of bortezomib was 18.4 mg/m2 (range, 11.4-41.6 mg/m2). The TB+ patients tended to interrupt bortezomib-containing therapy. Patients who interrupted bortezomib-containing therapy experienced MM progression within a few months. The best response rate was significantly lower in the TB+ group (Table 1). The median duration of follow-up for all patients was 21.1 months (range, 5.5-75 months). The median OS was 11.0±2.6 months (95% CI: 5.8-16.1 months) and 30.9±6.1 months (95% CI: 18.9-42.9 months) in the TB+ and TB- groups, respectively (P =0.017) (Fig. 1).
DISCUSSION
The treatment outcomes of novel agents for MM are promising, but these therapies are thought to have specific toxicities that differ from traditionally used agents. Bortezomib is known to have important adverse effects, including peripheral neuropathy, myelosuppression, and gastrointestinal disturbances. Heider et al. [6] reported a decline of CD4+ T cells in 77% of MM patients who were treated with bortezomib. In addition, the median CD4+ lymphocyte count significantly declined in all patients. Considering these results, the occurrence of herpes zoster in patients with MM treated with bortezomib could be explained by the decline in CD4+ counts. The effect of bortezomib treatment could potentially also influence the susceptibility of these patients to infections associated with low CD4+ T cells, such as M. tuberculosis infection [7]. We reviewed a large number of patients with MM who were treated with bortezomib-containing therapies. We found that the incidence of TB in bortezomib-treated patients (7%) was much greater than the annual incidence of TB in a general population aged 60-69 years (164.3 per 100,000 people) as reported by the Korea Centers for Disease Control and Prevention for 2007.
A limitation of our study was that bortezomib was administered in combination with other agents, and these agents may well have influenced patients' susceptibility to TB infection. Bortezomib was given in combination with thalidomide. Thalidomide is considered an adjuvant treatment for TB in some studies [11, 12], because it co-stimulates T lymphocytes and is thought to have a greater effect on CD8+ than on CD4+ T cells [13]. Bortezomib was also used with other immunosuppressant agents, specifically cyclophosphamide and dexamethasone. In this study, patients received low-dose cyclophosphamide (150 mg/m2 on days 1-4, every cycle). A previous study showed that low-dose cyclophosphamide selectively depletes CD4+CD25+ T cells [14]. Steroids are known to be an independent risk factor, and patients receiving a daily dose of ≥15 mg of corticosteroid for ≥1 month had an increased risk of developing TB [15]. To identify the influence of bortezomib on patients' susceptibility to TB infection, a direct comparison between patients who receive bortezomib and patients who receive steroid-containing salvage chemotherapy minus bortezomib is required [16].
In our study, 4 (50%) of the patients diagnosed with active pulmonary TB had interrupted consecutive treatment with bortezomib-containing regimens because of severe asthenia. This caused poor prognosis in all patients, even though 3 of the 4 patients showed a partial response to bortezomib-containing treatment at diagnosis with active pulmonary TB. In 2 patients, consecutive treatment of the bortezomib-containing regimen was interrupted for more than 5 weeks because of anti-TB treatment, and these patients showed disease progression within 5 months after initiation of an anti-TB regimen. The remaining 2 patients received continuous treatment for MM, and they were alive at the last follow-up. Patients with TB tended to receive fewer cycles of chemotherapy and lower bortezomib cumulative dosages compared with patients without TB, although statistical significance was not reached. We speculate that fewer cycles of chemotherapy and lower bortezomib cumulative dosages would affect best response rates and survival in MM patients with TB. Our findings emphasize that effective screening and early diagnosis for pulmonary TB infection are important in the treatment of MM patients. We propose that chest radiography screening should be performed prior to bortezomib treatment for the detection of healed or active pulmonary TB lesions. Even though skin testing with purified protein derivative of tuberculin (TST) is widely used to screen latent M. tuberculosis infection, it has relatively low sensitivity and specificityand is not possible to discriminate between latent infection and active disease. IGRAs are more specific than TST in terms of less cross-reactivity with BCG vaccination [1, 17]. Therefore, screening with IGRAs for patients with MM prior to bortezomib-containing chemotherapy should be considered in the diagnosis of latent tuberculosis. In addition, isoniazid prophylaxis should be given, if the IGRAs screening test results are positive. A key factor in the diagnosis of TB is a high degree of suspicion. If patients show pulmonary symptoms and have radiologic findings of atypical pulmonary infiltration during bortezomib-containing chemotherapy, active TB should be suspected and early diagnostic procedures such as sputum examination and chest CT should be performed.
 XML Download
XML Download