

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
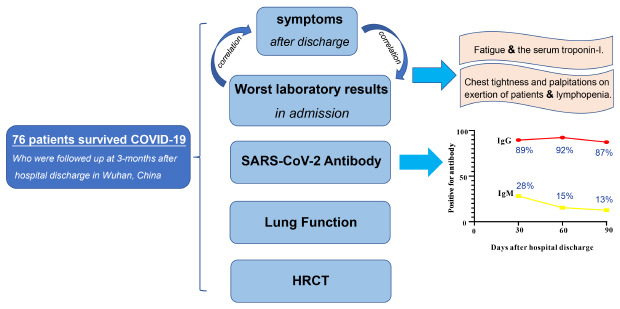
Outbreak of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome-coronaviruse-2 (SARS-CoV-2) in Wuhan, China, has been rapidly spreading nationwide and abroad. Up to July 24, 2020, over 15 million people have been infected with SARS-CoV-2 and more than 600,000 people died around the world.1 Wuhan, China was the first city to experience the COVID-19 pandemic. There were 50,333 people infected with SARS-CoV-2 and more than 2,000 health care workers (HCWs) including medical personnel, physicians, nurses and hospital workers are among those commonly infected.2 Epidemiological features and clinical characteristics of COVID-19 have been previously reported during the acute infection3 and most patients including health care workers survived COVID-19, however, our knowledge about the sequelae of COVID-19 remains limited. Hence, a further requirement for the identification and quantification of morbidity among survivors is to understand the long-term effects of this condition and its treatment. Therefore, the goal of this study was to characterize 3-month outcomes including the symptoms, pulmonary function, dynamic changes of SARS-CoV-2 antibody and high resolution computed tomography (HRCT) of patients who survived COVID-19 in the three months after discharge in Wuhan Union Hospital, China, in a prospectively observational follow-up study.
METHODS
Study design and patient selection
This is a prospective observational follow-up study of survivors of COVID-19 who were discharged from Wuhan Union Hospital, Wuhan, China. All patients enrolled in this study were confirmed by Nucleic acid testing (tested by reverse transcription PCR) of SARS-CoV-2 RNA in nasal/oropharyngeal swab samples and had met the criteria for discharge.4 Three nucleic acid tests for SARS-CoV-2 were performed during follow-up within three months after hospital discharge. Survivors were eligible for enrolment if they were ≥ 18 years old, but they were excluded if they had a history of pulmonary resection or had a documented neurological or psychiatric disease.
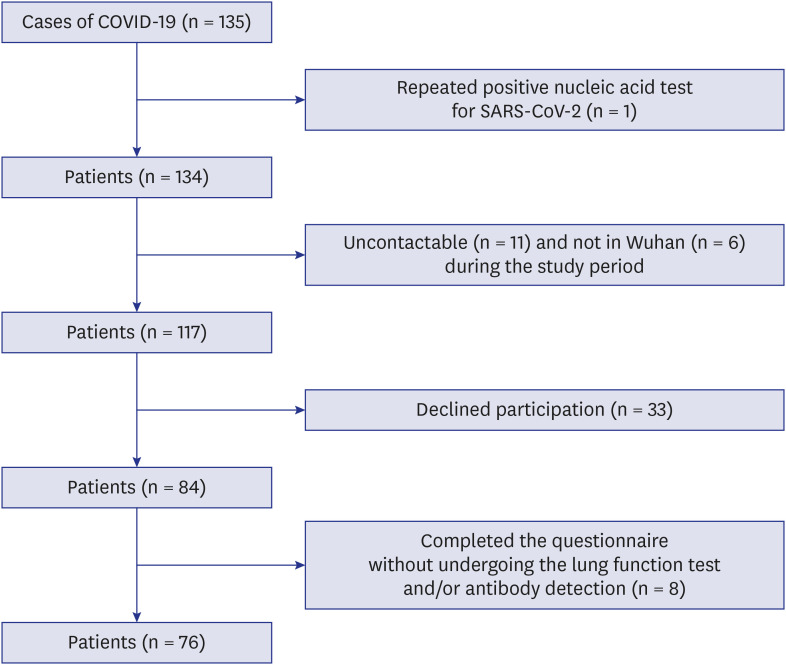
A total of 135 survivors of COVID-19 in Wuhan Union Hospital were evaluated in our study. Fifty-nine (44%) of 135 patients were excluded from our study for the reasons presented in Fig. 1. We also collected acute clinical data from the 76 hospitalized patients, which used a standardized data collection form as described previously by us5. During follow-up, each patient was interviewed using a standard questionnaire that evaluated persistent symptoms of patients after hospital discharge. Items such as cough, expectoration, chest tightness on exertion, palpitations, fatigue and diarrhea were assessed. We also collected serum samples to test IgG and IgM antibodies against SARS-CoV-2 at 1-month, 2-months and 3-months after hospital discharge, we also conducted the pulmonary function tests (PFTs) at 3-months after discharge. Some patients also underwent lung HRCT after discharge.
Pulmonary function testing
Pulmonary function tests were performed at the lung function laboratory at the Union Hospital during follow-up at 3-months after hospital discharge. Pulmonary function tests included spirometry, and measurements of total lung capacity (TLC), diffusing capacity of the lung for carbon monoxide (DLCO) and carbon monoxide diffusion constant (DLCO/VA). Lung function tests were measured using Yeage Masterscreen spirometer (German). Spirometries (forced expiratory volume in 1 second [FEV1] and forced vital capacity [FVC]) were performed according to the standards of the American Thoracic Society (ATS).6 If obstruction was present, the measurement was repeated after the administration of bronchodilator (salbutamol 400 μg) and the repeated measurement was used for analysis. TLC and its subdivisions were measured by the nitrogen washout method with the spirometer, adhering to standard criteria.7 DLCO and DLCO/VA were determined by the single breath technique using an infrared analyzer.8 DLCO was adjusted for the haemoglobin concentration evaluated within two weeks of the PFT. The spirometry, lung volumes, DLCO and DLCO/VA measurements were expressed as the percentages of predicted normative lung function values.
We investigated the correlations between shortness of breath score and pulmonary function data. We graded dyspnea into different scores according to a previous description.9 Dyspnea score was graded from one to four (one = dyspnea with strenuous activity, two = dyspnea with mild activity, three = dyspnea with minimal activity, four = dyspnea at rest or while eating or talking, respectively). In our study, patients without dyspnea were denoted by zero.
HRCT evaluation
HRCT images were assessed by one radiology and one pulmonary specialist at the same time together. The findings of parenchymal bands, irregular interfaces, traction bronchiectasis and architectural distortion were considered to be evidence of fibrosis changes.10 The worst HRCT Scores in the acute stage and the last HRCT scores in the follow up stage were also assessed similarly to one described previously11 and each lung was divided into three zones; each zone was evaluated for percentage of lung involvement. Summation of scores from all six lung zones provided the overall computed tomography (CT) score (maximal CT score, 24). Final scores were determined by an average of scores assessed by the two observers with a difference within 5%.
SARS-CoV-2 IgM and IgG GICA
The serum samples of the survivors were collected at 1-month, 2-months and 3-months after discharge to test SARS-CoV-2 IgG and IgM antibodies by gold immunochromatography assay (GICA) (SARS-CoV-2 IgG and IgM GICA kits, Livzon Inc, Zhuhai, P.R. China) following manufacturer instructions. Briefly, 15 μL aliquot of the serum was added to the specimen diluent and mixed. Aliquots of 80 μL diluted samples were pipetted into the sample wells of the SARS-CoV-2 IgG or IgM GICA cassette and the results were read within 20 minutes. The serum was considered positive if bands could be visualized on both the test and control lines. Each sample was repeated in triplicate.
Statistical analyses
SPSS 22.0 software (Chicago, IL, USA) was used for all analyses. Descriptive analysis results were reported as the mean ± standard deviation or as medians (interquartile ranges) for continuous variables and as proportions for categorical variables. We used two-sample t tests or the Mann–Whitney U test to compare continuous variables across groups and Pearson's chi-squared test (χ2) to compare categorical variables across groups. The risk factors of impaired pulmonary function at 3-months after discharge were evaluated using a multivariable linear regression model including age, sex, comorbidities, disease severity status, treatment in hospitalization (including corticosteroid prescription, antiviral and high-flow nasal cannula/noninvasive mechanical ventilation, highest level of LDH, worst CT score during acute illness and length of hospital days. We also calculated Spearman correlation coefficients for the relationships between worst laboratory results in admission and symptoms. Besides, we also calculated spearman correlation coefficients for the relationships between factors including worst LDH and HRCT score in acute illness, disease severity status, comorbidities and treatment in admission between PFTs and HRCT outcomes at 3-months after discharge. All statistical tests were two-tailed, and P < 0.05 was considered statistically significant.
RESULTS
Demographics and characteristics
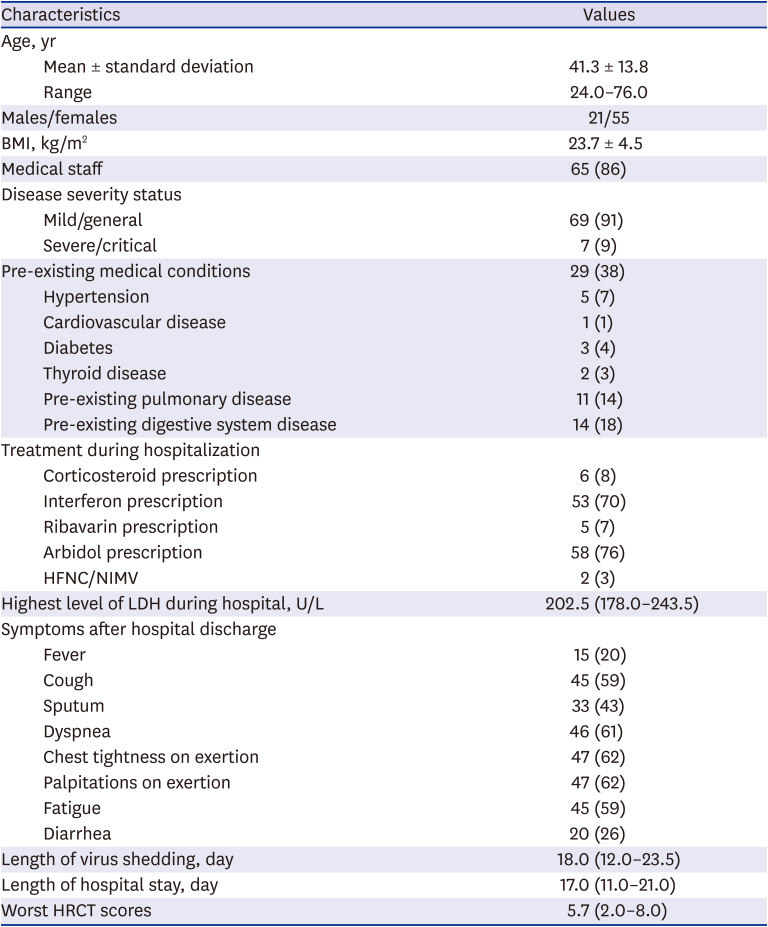
There were 76 survivors of COVID-19 enrolled in the study, and 55 (72%) were females, the median age was 41.3 ± 13.8 years (age range, 24 to 76 years). The mean body mass index was 23.7± 4.5. 65 (86%) survivors were healthcare workers and a total of 69 (91%) patients had returned to their original work during the observed time. Overall, 29 (38%) of 76 patients had pre-existing medical conditions and none of the survivors had history of smoking. The most common pre-existing illnesses were chronic gastritis, pulmonary tuberculosis, hypertension and diabetes mellitus. Pre-existing pulmonary diseases were noted in 11 (14%) patients as follows: five cases had treated pulmonary tuberculosis, three cases had chronic bronchitis and two cases had bronchial asthma. Although seven (9%) survivors were admitted to the intensive care unit (ICU), none of the patients required invasive mechanical ventilation. The median hospitalization time was 17 days (interquartile range [IQR], 11.0–21.0) and the median duration of SARS-CoV-2 virus shedding was 18 days (IQR, 12.0–23.5). Most patients received arbidol, interferon treatments, but only six (8%) cases received steroids during the acute phase of the illness, the details of demographics and characteristics of survivors enrolled in this study were showed in Table 1.
Table 1
Characteristics of the patients with COVID-19 (n = 76)
Symptoms during 3 months after discharge
During follow-up in the 3 months after hospital discharge, 15 (20%) patients had fever, 45 (60%) patients complained of cough, 33 (43%) had increased sputum production, 47 (62%) had activity chest tightness and palpitations, 45 (60%) complained of fatigue and 20 (26%) patients had diarrhea (Table 1). The worst serum troponin-I (TNI) levels during the acute illness showed high correlation with the symptom of fatigue after hospital discharge (correlation coefficient 0.782; P = 0.008) (Table 2). Low lymphocyte counts during the acute illness also showed significant correlation with the symptoms of chest tightness and palpitations on exertion of patients after hospital discharge (correlation coefficient: −0.285, P = 0.027; correlation coefficient: −0.363, P = 0.004, respectively) (Table 2). AST and ALT levels during the acute illness were positively correlated with fever after discharge. Besides, AST level and CD4 cells count in the acute illness were also positively correlated with diarrhea after discharge. Correlations between symptoms after hospital discharge and worst laboratory results during admission are shown in Table 2.
Table 2
Correlation between symptoms after hospital discharge and worst laboratory results in admission (n = 76)
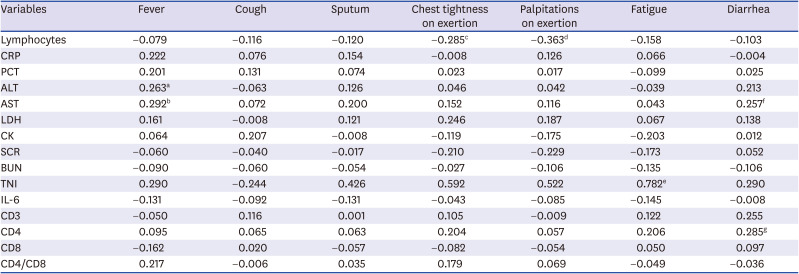
Data are Spearman correlation coefficients.
ALT = alanine aminotransferase, AST = aspartate aminotransferase, BUN = blood urea nitrogen, CRP = C-reactive protein, CK = serum creatine kinase, CD3 = CD3 (+) T lymphocytes, CD4 = CD4 (+) T lymphocytes, CD8 = CD8 (+) T lymphocytes, IL-6 = interleukin-6, LDH = serum lactic dehydrogenase, PCT = procalcitonin, SCR = serum creatinine, TNI = serum troponin-I.
a-gIndicate statistical significance (P < 0.05), aP = 0.042; bP = 0.023; cP = 0.027; dP = 0.004; eP = 0.008; fP = 0.047; gP = 0.037. P values are calculated by Spearman rank correlation tests. P value < 0.05 is considered to be statistically significant.
Pulmonary function tests
The mean values of FEV1, FVC, FEV1/FVC, TLC and diffusion capacity (DLCO and DLCO/VA) were all within normal limits (> 80% predicted) (Supplementary Table 1). However, some cases (32, 42%) with abnormalities in FEV1, FEV1/FVC ratio and DLCO were detected. Table 3 shows the pulmonary function data of 32 patients who had pulmonary function abnormalities. According to the ATS recommendations for evaluating respiratory impairment,12 four (5%) had mild impairment of FEV1, 17 (22%) had mild impairment of FEV1/FVC and 15 (20%) had mild impairment of DLCO. As shown in Table 3, among the 32 patients with impaired pulmonary tests, 15 (47%) had decreased DLCO levels with an average of 73.5 ± 4.3% and five had obstructive abnormality with a FEV1/FVC ratio < 70% predicted. Among patients who had pulmonary function abnormalities, nine patients had a history of medical illnesses that may affect pulmonary function. These included treated pulmonary tuberculosis, chronic bronchitis, bronchial asthma and thyroid diseases. All of these conditions were either well controlled or stable at the time of testing during our study. Among the five patients with obstructive abnormality, three had pre-existing medical conditions (patient 6, 11 and 23 in Table 3), however, two of the five patients had no comorbidity that would account for the abnormal lung function results. After excluding the above nine patients with history of medical illnesses that may affect pulmonary function, there were a total of 21 patients (27%) with impaired lung function at 3-months after discharge of COVID-19. However, because there is no data on lung function before these patients contracted COVID-19, it is still unclear whether these abnormalities may have existed before the diagnosis of COVID-19. Although the level of LDH and HRCT scores in the acute illness stage were higher in the PFT impaired group than that in the normal PFT group, the characteristics of patients with or without impaired PFT at 3-months after discharge were not statistically significant between the two groups (Supplementary Table 2). Interestingly, Spearman correlation coefficients showed that the HRCT score in acute illness was associated with PFT impairment (r = 0.229, P = 0.047). Multivariate analysis found that none of the prognostic factors (including age, sex, comorbidities, disease severity status, treatments in hospitalization, highest level of LDH, worst CT score during acute illness and length of hospital days) were significantly associated with the impaired lung function tests at 3-months after discharge (Supplementary Table 3). In accordance with the ATS recommendations,12 five patients received a bronchodilator and postbronchodilator spirometry values were used in the analysis.
Table 3
Clinical, pulmonary function data and HRCT of patients with impaired pulmonary function at 3-month after discharge (n = 32)
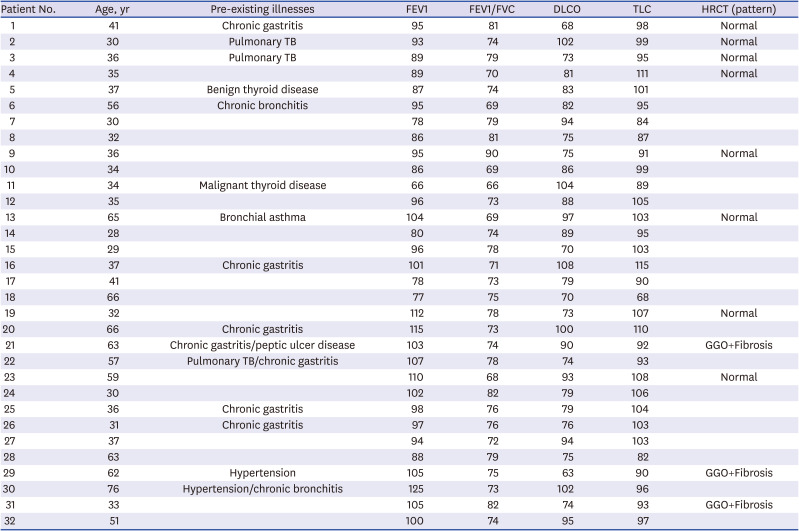
Pulmonary function data are presented as percentages of predicted values except FEV1/FVC, which is a percentage.
HRCT = high-resolution computed tomography, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, DLCO = carbon monoxide diffusing capacity, TLC = total lung capacity, TB = tuberculosis, GGO = ground-glass opacity, GGO+Fibrosis = ground-glass opacity with fibrosis.
In addition, dyspnea scores correlated well with measurements of a panel of pulmonary function parameters for FEV1, FVC, FEV1/FVC, TLC (P < 0.001, P < 0.001, P = 0.003, P < 0.001, respectively), providing validation for the scoring system used in our study (Table 4). Results of mean values of all measured functional parameters for different groups were listed in Table 4.
Table 4
Comparison of pulmonary function measurements among four different grades of dyspnea scores (n = 76)

Data are presented as mean ± standard deviation.
P values are calculated by Mann-Whitney U test. P value < 0.05 is considered to be statistically significant. Pulmonary function data are presented as percentages of predicted values except FEV1/FVC, which is a percentage.
FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, TLC = total lung capacity, VC = vital capacity, DLCO = carbon monoxide diffusing capacity.
Lung HRCT images after discharge
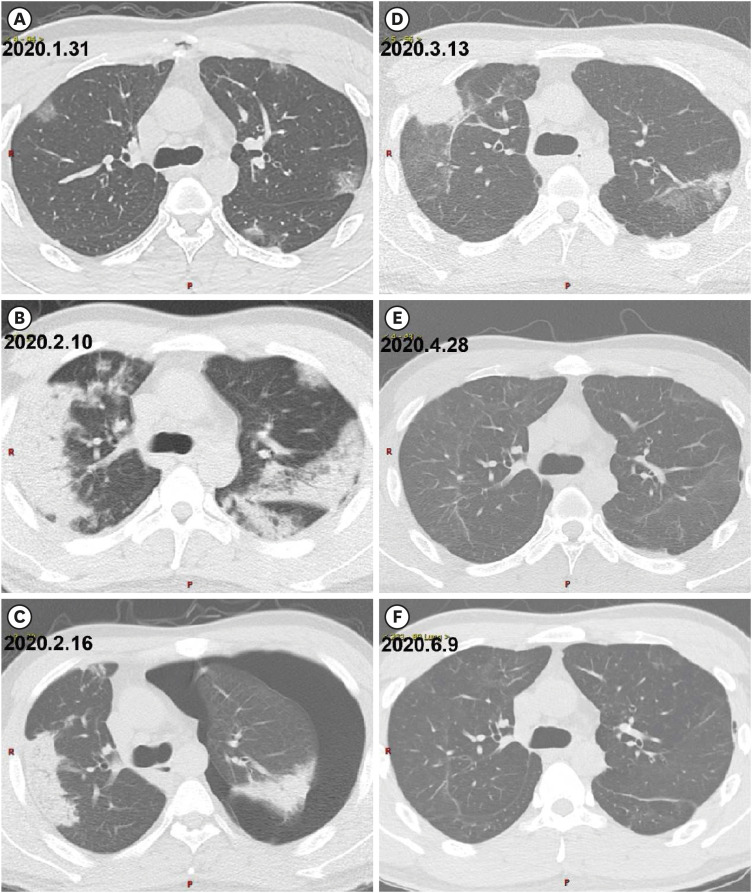
Lung HRCT was performed in 61 patients at 1-month or more after hospital discharge. We used the last HRCT of every patient to analyze, and the results showed that lung HRCTs returned to normal in most of the patients (50/61, 82%) at 3-months after discharge (Supplementary Table 4). Among the 21 patients who underwent HRCT examinations at 3-months after hospital discharge (3 months ± 1 week), five patients showed abnormalities on the HRCT imaging, including two patients with local ground-glass opacification (GGO) and three patients with both local GGO and fibrosis. Notably, among the 21 patients who took the HRCT at 3-months after discharge, there were eight patients with normal HRCT who showed impaired lung function tests at the same 3-months after discharge, however, two patients with only local GGO in HRCT had normal lung function. However, those patients had lower HRCT scores after discharge than that in hospital. There were no factors, including the worst HRCT score in the acute illness, significantly correlating with the outcome of HRCT resolution at 3-months after discharge. Fig. 2 showed the dynamic changes of lung HRCT of a patient with severe COVID-19 pneumonia and pneumothorax, and the results demonstrated the lung lesions and pneumothorax had improved gradually over time.
Fig. 2
HRCT scan of a 32-year-old patient with coronavirus disease 2019 obtained from January 31, 2020 to June 9, 2020 (the patient discharged on March 13, 2020). (A) Axial HRCT image shows bilateral, multifocal GGO that was predominantly located in the subpleural area. (B) Axial HRCT image shows bilateral, extensive area of consolidations that was distributed in the middle and outer zones. Air bronchograms have been seen. (C) Axial HRCT image shows that the consolidations became resolved and there was left pneumothorax. (D) Axial lung computed tomography image shows bilateral patchy areas of GGO with evidence of fibrosis. The area of consolidations continued to reduce. (E) Axial HRCT image shows that consolidations almost disappeared. The density and area of GGO were reduced, while fibrotic changes increased. (F) Axial HRCT image shows that GGO and fibrosis in bilateral lung lobes continued to resolve and gradually reduced.
HRCT = high-resolution computed tomography, GGO = ground glass opacity.
Dynamic changes of SARS-CoV-2 IgG and IgM antibodies
There were 57, 52 and 55 survivors tested for IgG and IgM antibodies against SARS-CoV-2 at 1-month, 2-months and 3-months after discharge, respectively. Supplementary Fig. 1 shows the dynamic changes of survivors with positive SARS-CoV-2 IgG and IgM during the three months after hospital discharge, and the results showed that SARS-CoV-2 IgG turned negative in 11% (6 of 57 patients), 8% (4 of 52 patients) and 13% (7 of 55 patients) at 1-month, 2-months and 3-months after discharge, respectively, and SARS-CoV-2 IgM turned negative in 72% (41 of 57 patients), 85% (44 of 52 patients) and 87% (48 of 55 patients) at 1-month, 2-months and 3-months after discharge, respectively. It's worth noting that both IgM and IgG antibodies were undetected from the illness onset to three months after discharge in two patients with mild COVID-19 (2/76, 3%).
DISCUSSION
Our results showed that infection by SARS-CoV-2 had some mild impacts and impairments on survivors of COVID-19 after their discharge, but the impacts and impairments were mild in almost all cases, and most survivors returned to their original work during the three-months after their discharge from hospital.
Most survivors of COVID-19 had symptoms including fever, sputum production, fatigue, diarrhea; and more than half of the survivors had dyspnea, cough, chest tightness and palpitations on exertion in the three months after discharge even though the lung lesions were resolved completely in lung HRCT, which demonstrated SARS-CoV-2 infection can cause persistent damage that may be due to pulmonary and/or extrapulmonary disease. As we know, SARS-CoV-2, the causative agent of COVID-19, has been shown to cause persistent damage of the heart, intestine, kidney and pulmonary system by a direct effect owing to viral replication in the organ cells and indirect damage secondary to respiratory failure or an exaggerated immune system response.131415 That damage induces symptoms in the acute stage, and may also in the sequel stage. A previous study16 revealed cardiac involvement in 78% of German patients recovered from COVID-19 and ongoing myocardial inflammation in 60% of all patients, independent of preexisting conditions, severity and overall course of the acute illness, and time from the original diagnosis, which indicates COVID-19 can cause persistent damage even in the sequel stage. It is interesting that our results show that the troponin I level is related to fatigue and the lymphopenia is associated with chest tightness and palpitation on exertion. Previous studies171819 showed that myocardial injury occurs in a significant proportion of COVID-19 patients and the cardiac TNI or troponin-T which is the sensitive marker of myocardial injury and an independent predictor of clinical outcomes in the acute stage20 is also associated with heart damage in the recovery stage of COVID-19.16 Lymphopenia, as a prognostic factor affecting the prognosis of COVID-19 is associated with cytokine storm which is one of the most important causes of multi-organ injury.2122 Our study indicates that the degree of lymphopenia in the acute stage could also be a prognostic factor affecting the rehabilitation of COVID-19. In our observation, the impact of symptoms on survivors of COVID-19 were mild in almost all cases, and most survivors returned to their original work during the three-months post discharge. This may be due to the mostly mild, as well as general, cases in our study and the observation of the long-term sequelae of SARS-CoV2 infection especially in severe patients in the future is needed.
Although the mean values of FEV1, FVC, FEV1/FVC, TLC and diffusion capacity (DLCO and DLCO/VA) were all within normal limits (> 80% predicted), we found that about 42% (32/76) of survivors had impaired respiratory capacity (FEV1, FVC, DLCO), in the meantime, dyspnea scores correlated well with measurements of the above function parameters for FEV1, FVC, FEV1/FVC and TLC, which demonstrated COVID-19 pneumonia can cause persistent impaired pulmonary function for some time after discharge, and cause some of the symptoms such as dyspnea. However, the proportion of patients with impaired lung function tests were less than the previous studies investigating the effects of severe acute respiratory syndrome (SARS) infection on pulmonary function23, this may be due to more patients showing mild symptoms in our cohort. It is worth mentioning that lung lesions in HRCT were absolutely resolved in most patients after discharge at three months, however, the pulmonary function was impaired in some patients with normal lung HRCT at three months, this result indicates the pulmonary function test was more sensitive for lung rehabilitation after SARS-CoV-2 pneumonia than that of HRCT. Previous reports had showed that severe pneumonia significantly impairs pulmonary function and makes long radiological sequelae at the 1-year follow-up prospective cohort study about MERS survivors.24 Additionally, patients who required ICU admission had significantly lower FVC, TLC, and TLCO at 6 months after discharge25 and only the use of pulse steroids was found to be an independent factor associated with the presence of CT abnormalities in another study about SARS survivors.26 This study also indicates that, compared to the normal lung function group at three months after discharge, the lung function impaired group has higher HRCT scores and worse LDH levels, in the acute illness phase and the worst HRCT score was significantly correlated with impairment of lung function. However, differences between the two groups are not statistically significant, which may be due to the small number of cases, especially small cases of critically ill patients, which suggests that it is necessary to enroll more cases, especially critical cases, to observe the impact of disease severity on pulmonary rehabilitation. In the investigation of the sequelae of survivors of SARS, persistent pulmonary function impairments were found in some patients at 12 months after discharge,2728 or even through 24 months after discharge, and a gradual improvement of pulmonary function had also been seen.29 In addition, acute respiratory distress syndrome patients showed that all the lung volume and spirometric measurements and carbon monoxide diffusion capacity become normal within one year after discharge.30 In our cohort, the lung lesion of a patient with severe pneumonia and pneumothorax improved gradually, only leaving mild GGO and fibrosis in lung HRCT and mild disfunction of pulmonary diffusion at three months after discharge. Combined with the results above, this suggests the lung damage caused by SARS-CoV-2 infection may gradually recover.
The IgM antibody turned negative after discharge at one month in most patients, and the duration of IgG antibody remained positive at 3-months after discharge in most patients, however, the percentage of patients with positive serum IgG antibodies decreased gradually (undetectable in 11% [6/57], 8% [4/52], 13% [7/55] at 1-month, 2-months and 3-months after discharge, respectively). This was consistent with previous studies on SARS-CoV-2 infection, which had found that both IgM and IgG antibodies against SARS-CoV-2 were detected as early as the 4th day after symptom onset, and the seropositive rate of IgG was observed decreased around the 28th day after illness onset.31 Those results indicate the longevity of IgG antibody in those patients with SARS-CoV-2 infection was shorter than SARS and the Middle East respiratory syndrome (MERS), another two severe coronavirus pneumonia, in which serum IgG antibodies against SARS-CoV maintained seropositive (100%) within the first 16 months of illness,32 although antibody titers gradually waned. The antibody titers of IgG against MERS–CoV were observed waned at one year after disease onset.33 It's worth noting that both IgM and IgG antibodies were undetected from the illness onset to discharge from hospital at three months in two patients with mild COVID-19. A previous study on MERS-CoV infection indicated that serologic responses to MERS-CoV virus were variable, and often undetectable in mild patients.33 There is also a report of undetected IgM and IgG against SARS-CoV-2 in a renal transplant recipient with COVID-19 for more than two months after illness onset.34 These data indicate that immunosuppressive status or milder infections are less likely to elicit serologic responses. However, the mechanism of undetectable SARS-CoV-2 antibodies against SARS-CoV-2 in those patients remains unknown.
There are several limitations of our current study. First, our study had a limited number of patients and the majority (91%) of enrolled patients had mild COVID-19, therefore the favorable prognosis could be due to the lack of severe cases in this study. In addition, this study enrolled only 76 patients in Wuhan Union Hospital and thus the results may not be representative of all convalescent individuals in this or other countries. Second, a portion of patients who declined participation might have led to a selection bias. It is likely that the patients who declined participation may have done so because they were asymptomatic or felt inconvenienced by the study. Third, because some patients had no prior medical history, we could not confirm if their lung function abnormalities were newly developed or existed before their COVID-19 diagnosis. Fourth, our study does not provide data on the titers of serum IgG and IgM antibodies against SARS-CoV-2. Fifth, not all enrolled patients performed HRCT examinations during the 3-month follow-up period after hospital discharge. Some patients who were not symptomatic could not be scanned for HRCT. Sixth, evaluations of the damage to the heart and myocardium such as electrocardiogram, 24-hour Holter monitoring, myocardial enzyme testing and cardiac magnetic resonance imaging that may be correlated with symptoms were not performed after discharge from hospital. However, serum TNI and myocardial enzymes were normal when patients discharged from hospital. Finally, although mental health burden and neuromuscular function may affect or account for symptoms of survivors that were present after hospital discharge, assessments of them were not performed in this study.
In conclusion, most of the survivors returned to their original work in the three months after discharge. However, more than half of survivors of COVID-19 had mild symptoms in the three months after discharge. The troponin I level in the acute illness was related to fatigue and the lymphopenia was associated with chest tightness and palpitation on exertion. Besides, the impaired pulmonary functions were detected in 42% of the recovered COVID-19 patients at 3-months after hospital discharge and were correlated with dyspnea scores. Additionally, the IgM antibody turned negative after discharge at one month in most patients, and the percentage of patients with positive serum IgG antibodies decreased gradually in the 3-months after discharge, suggesting the duration of SARS-CoV-2 antibodies was limited. The impact of symptoms after discharge and impairment of pulmonary functions as well as HRCT were mild in all cases in our observation. The favorable prognosis could be because the majority of our patients were mild cases. Those indicate SARS-COV-2 infection may cause persistent pulmonary and/or extrapulmonary damage, and the observation of the long-term sequelae of SARS-CoV2 infection especially in severe patients in the future is needed.
 XML Download
XML Download