

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The mortality rate following neurosurgical treatment of an unruptured cerebral aneurysm varies from 0.4% to 1.5%, and age of the patient and size and location of the aneurysm are generally accepted factors that affect surgical outcome.9) For achievement of acceptable surgery-related morbidity and mortality rates, neurosurgeons strive for precise aneurysmal neck clipping, careful confirmation of branches or perforators that were not clipped together, and maintenance of flow in the parent artery to prevent ischemic accidents. Atherosclerotic changes in the intracranial artery and in part of the aneurysm result in diminished flexibility of the vessel itself, which not only makes the surgery difficult to perform but can also result in unexpected ischemic complications such as thromboembolism and vessel occlusion.2) In the current study, we analyzed and reported the clinical features of atherosclerotic intracerebral aneurysms treated at our center.
MATERIALS AND METHODS
Subjects
Cases of 262 patients who underwent aneurysmal neck clipping surgery at our center between June 2004 and November 2010 were analyzed retrospectively. We reviewed intraoperative videos; microscopic photographs; pre- and post-operative findings of computed tomography angiogram (CTA), magnetic resonance angiogram (MRA), and digital subtraction angiogram (DSA); and medical and surgical records. We divided the patients into two groups: the atherosclerotic group (AG) with atherosclerotic appearance of vessels, and the non-atherosclerotic group (NAG) without atherosclerosis.
Evaluation of atherosclerotic aneurysm
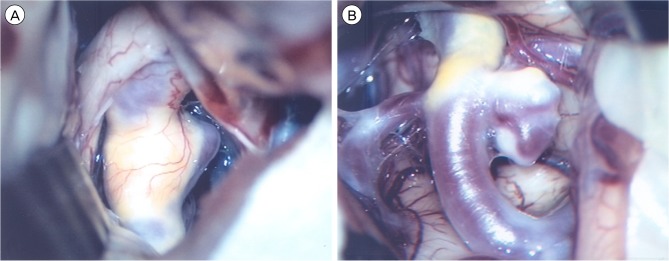
The criteria for atherosclerotic aneurysm were assessed according to the surgeons' intraoperative findings, either retrospectively or prospectively. Atherosclerotic changes in the vessel or aneurysm walls were identified as follows: (1) yellowish and/or whitish spotty appearance of the vessel and/or aneurysm; (2) surgical confirmation of a definite decrease in elasticity of the wall, with or without a color change of the vessel (Fig. 1).
Atherosclerosis types were divided according to the following categories based on the position of the atherosclerotic changes: (1) parent artery and aneurysm neck; (2) aneurysm neck; (3) aneurysm neck and dome; (4) aneurysm dome. Location in the parent artery was defined as atherosclerotic change within 5 mm from the neck of the aneurysm.
Evaluation of surgical result
Clinical outcome was determined according to scoring and changes on the Glasgow outcome scale (GOS). The outcome was determined as favorable if the GOS score was either unchanged, regardless of the preoperative status, or improved to a GOS score of 4-5. An outcome was considered unfavorable if there was deterioration to a GOS score of 1-3. In addition, the occurrence of new postoperative ischemia was assessed with a head computed tomography (CT) scan. The postoperative CT was analyzed for territory infarction or perforator infarction in relation to the clip position.
Statistical analysis
To evaluate the difference between the AG and NAG, the variables of clinical characteristics, aneurysmal characteristics, and surgical procedures between the two groups were compared using univariate methods (the two-sample t-test, Fisher's exact test, and Pearson's Chi-square test). MedCalc® (version 13, MedCalc Software bvba, Ostend, Belgium) was used for analysis, and a p value less than 0.05 was considered statistically significant for all statistics.
RESULTS
Patient characteristics
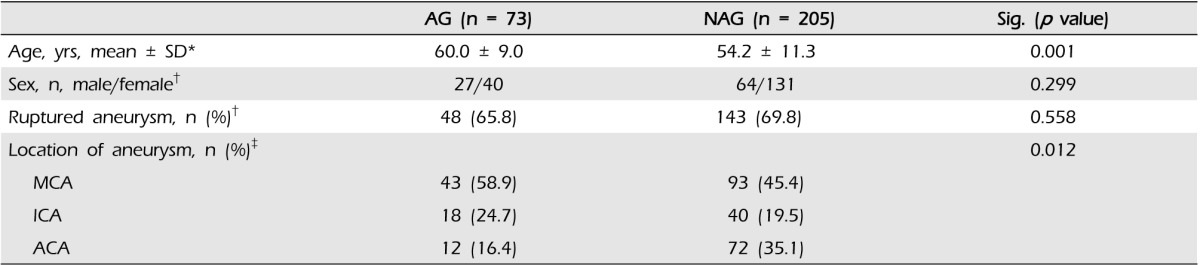
Among 262 patients who underwent aneurysm clipping surgery at our center between June 2004 and November 2010, atherosclerotic aneurysms were found in 67 patients, representing approximately 25.6% of all patients undergoing aneurysm clipping surgery. The mean age of the patients with atherosclerotic aneurysms was 60.0 ± 9.0 years (mean ± SD, range: 38-74), among whom 27 were males and 40 were females. The mean age of the remaining 195 patients without atherosclerotic aneurysms was 54.2 ± 11.3 years (mean ± SD, range: 21-79), among whom 64 were males and 131 were females (Table 1).
Characteristics of aneurysms
A total of 73 lesions were identified among the atherosclerotic aneurysms; of these, 48 lesions were ruptured and the remaining 25 were unruptured. Among the non-atherosclerotic aneurysms, 205 lesions were identified; of these, 143 and 62 were ruptured and unruptured, respectively.
Among the atherosclerotic aneurysms, 43 were found in the middle cerebral artery (MCA), 18 were found in the internal carotid artery (ICA), and 12 were found in the anterior cerebral artery (ACA). Among the non-atherosclerotic aneurysms, 93 were found in the MCA, 40 were found in the ICA, and 72 were found in the ACA (Table 1). A significant difference in aneurysm location was observed between the two groups (p = 0.012).
Characteristics of atherosclerotic changes
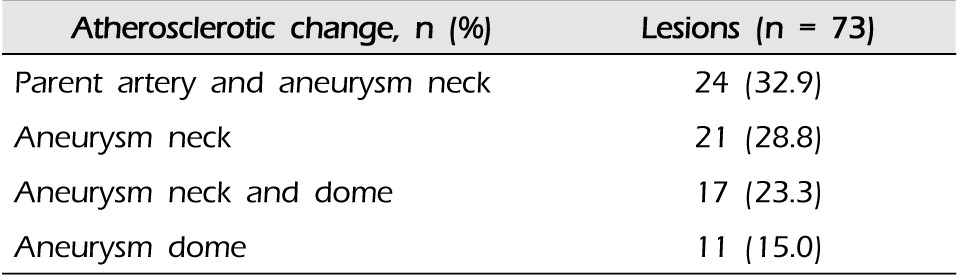
When the vessels with atherosclerotic changes were visualized intraoperatively, sites of the changes varied considerably. Atherosclerotic changes were observed in the parent artery and aneurysm neck in 24 cases, in the aneurysm neck in 21 cases, in the aneurysm neck and dome in 17 cases, and in only the aneurysm dome in 11 cases (Table 2).
Surgical procedure
Out of 73 atherosclerotic aneurysms, 14 were clipped with multiple permanent clips; however, remnant neck and clip slippage were later observed in six and four cases, respectively. Among 205 surgeries for non-atherosclerotic aneurysms, multiple clippings were performed in 34 cases, remnant neck was found in five cases, and clip slippage occurred in four cases. Comparison of the two groups showed a statistically significant difference in the variable of intentional remnant neck (Table 3). We then subdivided the specific surgical steps in the atherosclerotic aneurysm group; there were 15 cases of specific surgical steps in the group with atherosclerotic change in the parent artery and aneurysmal neck. Among them, multiple clippings were performed in seven cases, remnant neck was found in four cases, and clip slippage occurred in three cases, with only one case of wrapping. In another group, atherosclerotic change on the aneurysmal neck, multiple clippings were performed in six cases, remnant neck was found in two cases. In the other group, atherosclerotic change on the aneurysmal neck and dome, multiple clippings were performed in one case and clip slippage occurred in one case (Table 4).
Post-operative outcome
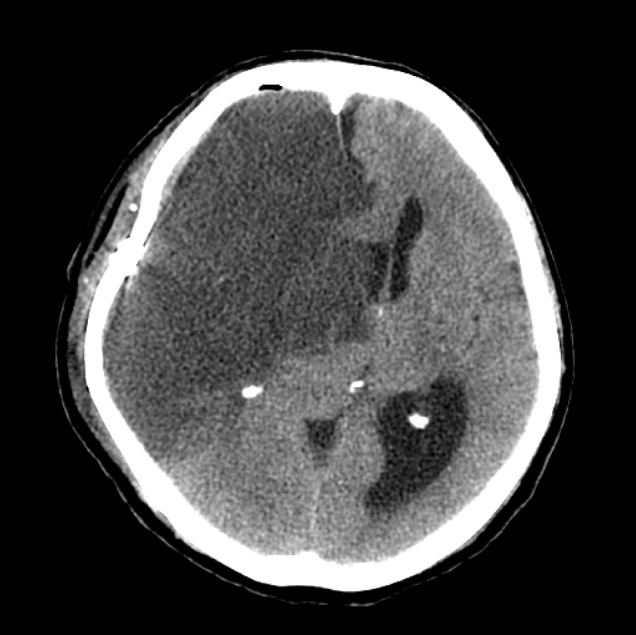
In review of the postoperative outcomes of patients in the AG, 47 patients had GOS score of 4-5 and 20 patients had GOS score of 1-3. One patient expired because of a territory infarction. In the AG, postoperative ischemic lesions developed in five patients; two of these patients had a total territory infarction (Fig. 2) and three patients had a perforator infarction related to the site of the operated lesion. In the NAG, five patients had infarctions in small subcortical regions. However, all patients in the NAG who developed postoperative infarctions recovered completely from their neurologic deficits. No statistical difference in development of ischemic complications was observed between the two groups.
DISCUSSION
Recently, treatment of cerebral aneurysms has been developing at a rapid pace, and a number of studies have reported good clinical outcomes of aneurysm surgeries. However, Flamm et al. reported that the presence of plaque in an aneurysm can be a predictive factor for unexpected complications during aneurysm surgery.3) Other researchers have also examined the importance of atherosclerotic aneurysms.
In 1999, Ohno et al. reported atherosclerotic changes in six patients (10%) among 30 patients with cerebral aneurysms.8) Similarly, in 2003, Grigorian et al. reported atherosclerotic changes in 81 patients (26.7%) among 333 patients with aneurysms.4) In our study, 67 (25.6%) of the 262 patients with aneurysms had atherosclerotic aneurysms. Therefore, when treating aneurysms, understanding the pathophysiology of atherosclerotic changes is important.
Atherosclerosis is a well-known pathological condition that generally affects the arterial blood vessels. As a degenerative process, atherosclerotic changes result from deposition of plasma lipids, connective tissues, and local or circulating cells over the intima of the blood vessels, which leads to narrowing of the vessel lumen.7) The restorability of such atherosclerotic vessels is limited because of a resultant decrease in elasticity and increase in rigidity of the vessel.10) During aneurysm surgery, if the aneurysmal neck has atherosclerotic changes, problems such as incomplete neck clipping and narrowing of the lumen of the parent artery may occur.8) In particular, narrowing of the lumen of the parent artery may be an important cause of postoperative ischemic events.
Regarding aneurysm location, Szelenyi et al. reported that among patients with atherosclerotic aneurysms, ten had aneurysms in the ICA, five had aneurysms in the anterior communicating artery, and 19 had aneurysms in the MCA.9) Ohno et al. reported that six patients among seven patients with atherosclerotic changes in the aneurysmal neck had MCA aneurysms.8) In our study, 43 patients among the 73 patients with atherosclerotic aneurysms had aneurysms in the MCA.
Szelenyi et al. reported that eight cases among 34 atherosclerotic aneurysm cases had atherosclerotic changes in the parent vessel, aneurysm dome, or aneurysm neck, respectively, and 11 cases had changes in both the aneurysm dome and neck.9) In our study of 73 cases, the sites of atherosclerotic change were as follows: both parent artery and aneurysm neck in 24 (32.9%), aneurysm neck in 21 (28.8%), both aneurysm neck and dome in 17 (23.3%), and aneurysm dome in 11 (15.0%). These findings are not relevant to the findings reported in the papers mentioned earlier.
Regarding the postoperative prognosis of patients with atherosclerotic aneurysms, Szelenyi et al. reported that 27 of 34 atherosclerotic aneurysm patients had a good clinical outcome, increasing to 30 patients at six months. Postoperatively, four patients had an unfavorable outcome, and at the six-month follow-up, only three patients had an unfavorable outcome.9) In our series, 47 patients had a favorable outcome, 20 patients had an unfavorable outcome, and, unfortunately, one patient expired. The most likely explanation for the higher rate of unfavorable clinical outcomes in our series as compared with that of Szelenyi et al. is that the latter study included only unruptured aneurysms, whereas we included 48 cases of ruptured aneurysms. Reviews of other studies have found that the frequency of morbidity in patients with atherosclerotic aneurysms is higher than in patients with non-atherosclerotic aneurysms, approximately 14% and 6.8%, respectively.2)3)6)
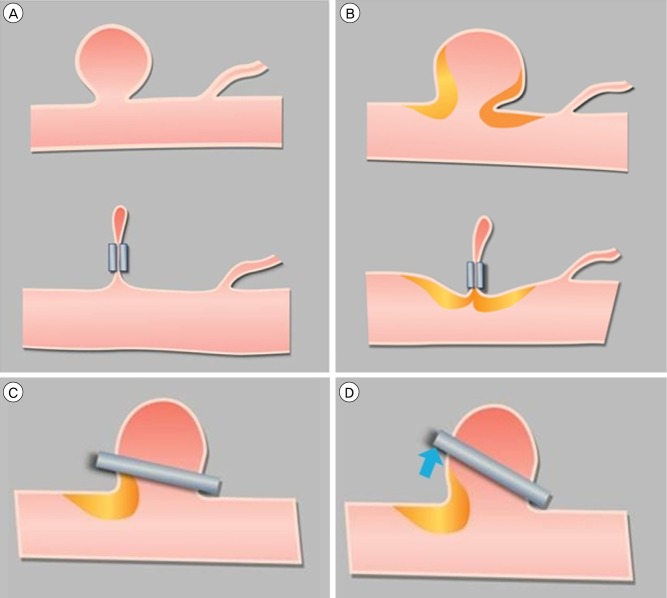
In atherosclerotic aneurysms, the atherosclerotic wall might increase the occurrence of thromboembolic events, or its rigidity might lead to occlusion of perforators within the aneurysm vicinity during surgery.1)5) Szelenyi et al. reported that in six patients with atherosclerotic aneurysms, a small residuum of the aneurysm neck was intentionally left. This was done significantly more often than in patients with non-atherosclerotic aneurysms. In addition, in patients with atherosclerotic aneurysms, temporary vessel occlusion and multiple repositioning of the permanent clip were performed more often than in patients with non-athe rosclerotic aneurysms. Although the application of more than one permanent clip and wrapping occurred more often in patients with atherosclerotic aneurysms, this did not reach statistical significance in their study.9) It is expected that clip placement in atherosclerotic aneurysms requires more surgical steps compared with non-atherosclerotic aneurysms. This is supported by our finding that the intraoperative observation of atherosclerosis showed significant correlation with a higher percentage of multiple positioning of a permanent clip. Clip placement might be hampered by a rigid atherosclerotic wall such that aneurysm obliteration due to sliding of the clip off the aneurysm dome is not complete or that the parent vessel or perforating branches are occluded (Fig. 3). One solution to this problem is aneurysm obliteration with multiple clips.8)9) Furthermore, as in our study, avoidance of the region of the atheroma could promote effective clip placement and prevent parent artery occlusion.
CONCLUSION
In the surgical repair of aneurysms, the incidence of ischemia, which is irreversible or severe, might be greater in atherosclerotic than in non-atherosclerotic aneurysms. Careful manipulation and a thorough understanding of atherosclerotic vessels during neck clipping surgery can prevent ischemic accidents resulting from parent artery stenosis or perforating artery occlusion and yield satisfactory surgical results. In addition, multiple clips might be applied to atherosclerotic aneurysms for effective obliteration and the aneurysm neck might be left to avoid a region of atheroma.


 XML Download
XML Download