

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
It is necessary to distinguish between pyogenic and tuberculous spondylitis of infectious spondylitis, if it is pyogenic spondylitis, antimicrobial therapy should be directed against an identified microorganism and clinical assessment should be done at 4 weeks. But if microorganism is a anaerobic bacteria, especially Peptostreptococcus anaerobius, combination antibiotic therapy should be considered bacause it may be a component of mixed infections as a passenger and have abilities to induce abscesses, other bacterial growth as a synergy effect. In addition, echocardiography may be necessary because pyogenic spondylitis is associated with infective endocarditis about 12%. We report a 64-year-old man who was treated for infectious spondylitis accompanied by Peptostreptococcus anaerobius bacteremia, but had to undergo heart surgery because an attack of infective endocarditis with systemic embolism during hospitalization.
Figures and Tables
Fig. 1
Spine MRI shows diffuse contrast enhancement of prevertebral soft tissue and endplate at L5-S1 (arrow).
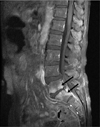
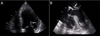
Fig. 2
Septic emboli identified according to imaging modalities (arrow). (A) Contrast-enhanced abdominal CT shows wedge shaped low attenuated lesion at spleen. (B) Aggravated state of spleen after 8 weeks. (C) Brain MRI shows acute ischemic infarct in both occipital lobe. (D) CT angiography of femoral artery shows focal segmental occlusion at distal portion of right popliteal artery.


References
1. Kim YI, Kim SE, Jang HC, Jung SI, Song SK, Park KH. Analysis of the Clinical Characteristics and Prognostic Factors of Infectious Spondylitis. Infect Chemother. 2011. 43:48–54.

2. Koo KH, Lee HJ, Chang BS, Yeom JS, Park KW, Lee CK. Differential Diagnosis between Tuberculous Spondylitis and Pyogenic Spondylitis. J Korean Soc Spine Surg. 2009. 16:112–121.
3. Gouliouris T, Aliyu SH, Brown NM. Spondylodiscitis: update on diagnosis and management. J Antimicrob Chemother. 2010. 65:iii11–iii24.
4. Murdoch DA. Gram-positive anaerobic cocci. Clin Microbiol Rev. 1998. 11:81–120.
5. Zimmerli W. Clinical practice. Vertebral osteomyelitis. N Engl J Med. 2010. 362:1022–1029.
6. Cottle L, Riordan T. Infectious spondylodiscitis. J Infect. 2008. 56:401–412.
7. Minces LR, Shields RK, Sheridan K, Ho KS, Silveira FP. Peptostreptococcus infective endocarditis and bacteremia. Analysis of cases at tertiary medical center and review of the literature. Anaerobe. 2010. 16:327–330.
8. Könönen E, Bryk A, Niemi P, Kanervo-Nordström A. Antimicrobial susceptibilities of peptostreptococcus anaerobius and the newly described peptostreptococcus stomatis isolated from various human sources. Antimicrob Agents Chemother. 2007. 51:2205–2207.
9. Lee KY, Chong YS, Jeong SH, Xu XS, Kwon OH. Emerging Resistance of Anaerobic Bacteria to Antimicrobial Agents in South Korea. Clin Infect Dis. 1996. 23:S73–S77.
10. The Korean Society of Infectious Diseases. Korean Society for Chemotherapy. The Korean Society of Clinical Microbiology. The Korean Society of Cardiology. The Korean Society for Thoracic and Cardiovascular Surgery. Clinical Guideline for the Diagnosis and Treatment of Cardiovascular Infection. Infect Chemother. 2011. 43:129–177.
 XML Download
XML Download