

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Cleidocranial dysplasia (CCD) is a rare congenital bone disease characterized by abnormalities of the clavicles, skull, and jaw, as well as occasional stunting of long bones.12 The clavicles are typically hypoplastic or display unilateral or bilateral discontinuity, and in about 10% of cases, they are completely absent.1 Mutations in the runt-related transcription factor 2 gene are responsible for approximately two-thirds of CCD cases.2 This gene normally guides osteoblastic differentiation, chondrocyte maturation, and appropriate bone formation.2 It also plays an important role in the epithelial-mesenchymal interactions that control progressive tooth morphogenesis and the histodifferentiation of the epithelial enamel organ.3
The gnathic and dental features of CCD are distinctive and may lead to an initial diagnosis in most CCD cases.1 Dental dysplasia manifests as the presence of multiple supernumerary teeth, the prolonged retention of deciduous teeth, and the delayed or failed eruption of the permanent dentition.4 The causes of delayed eruption of permanent teeth are still under debate, but potential options include the presence of supernumerary teeth in the eruption pathway,5 the presence of a dense alveolar crest,16 the lack of cellular cementum of the permanent teeth,7 and the reduced ability of periodontal ligament cells to induce osteoclastic differentiation.8
Many case reports of CCD patients have been published,4 but few studies have focused on long-term radiographic analysis of tooth eruption in CCD patients. In addition, no reports have been published on the effect of time on the impacted teeth of CCD patients with or without dental interventions, including extraction or orthodontic treatment. Understanding this relationship is highly clinically significant to the decision-making process about dental treatment and could improve the quality of life of CCD patients.
This report described 3 cases of CCD patients, focusing on the eruption status of impacted permanent teeth as shown on long-term follow-up radiographs. The follow-up periods were 3, 13, and 13 years, respefctively.
Case Report
Case 1
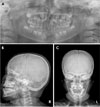
A 7-year-old girl visited our department of orthodontics complaining of maxillary hypoplasia in 2016. The 32-year-old mother of this child also had CCD. Due to the family history, the parents were prepared for the possibility that their child had CCD, and they had scheduled regular visits at a dental hospital. Underdevelopment of the clavicle (deficient clavicles) was observed on a chest radiograph taken 6 years prior at a medical hospital (Fig. 1).
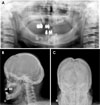
A panoramic radiograph was obtained and revealed delayed eruption of multiple permanent teeth and a small radiopaque body above the dental follicle of the right lower canine (Fig. 2A). The radiopaque body exhibited a structure resembling that of a tooth and was found to be an impacted supernumerary tooth. Elective removal of this supernumerary tooth was performed because the tooth could otherwise prevent the eruption of the right lower canine. When the patient was 8 years old, partial orthodontic treatment was begun for maxillary anterior crowding, which was the chief complaint of the patient and her guardians. Lateral and posteroanterior skull radiographs were taken to evaluate the bony structures of the craniofacial region; these revealed characteristic features, including hypoplasia of the maxilla, Wormian bone in the cranial suture, and parietal bossing (Figs. 2B and C).
When the patient was 10 years old, another panoramic radiograph was obtained for re-evaluation of her dentomaxillofacial status (Fig. 3). It revealed 3 newly formed supernumerary teeth, all of which were found between the canine and first premolar of the upper right, upper left, and lower left regions.
When the patient was between 7 and 10 years of age, the upper and lower premolars had almost erupted due to extraction of the overlying supernumerary teeth and orthodontic treatment. After the patient underwent proper orthodontic treatment, panoramic radiography showed normal eruption patterns.
Case 2
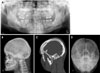
A 23-year-old man visited our dental hospital in 2005 complaining of delayed eruption of permanent teeth. Several radiographic images of the patient were obtained in order to make an accurate diagnosis. A panoramic radiograph (Fig. 4A) showed multiple impacted permanent teeth and prolonged retention of numerous deciduous teeth. Supernumerary teeth were observed on the distal side of the left upper third molar and above the right lower first premolar. The lateral skull view and the sagittal view on cone-beam computed tomography (CBCT) showed maxillary hypoplasia and the presence of Wormian bone in the rhomboidal suture (Figs. 4B and C). Waters' view (Fig. 4D) showed downward displacement of the zygomatic arch, a small maxillary sinus, parietal bossing, and a large anterior fontanelle. Orthodontic treatment, including extraction of supernumerary teeth, was planned, but at that time, the patient did not receive adequate dental care.
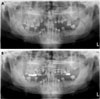
After 12 years, the same patient visited our dental hospital with the same chief complaint. A panoramic radiograph (Fig. 5A) showed similar radiological characteristics, including multiple impacted permanent teeth, supernumerary teeth, and sclerosis of tooth-bearing alveolar bone. Many deciduous teeth were retained with the corresponding permanent teeth absent, and generalized periodontal bone loss was evident. Some teeth displayed slight eruption, but most were still impacted despite the 12-year period that had elapsed. Some teeth seemed to have erupted, not due to a healthy eruption process, but because of the loss of surrounding alveolar bone and numerous deciduous and permanent teeth. The exception was the lower second premolars on both sides, which had erupted to the occlusal level.
Dense alveolar bone was observed around both lower premolar regions. A coronal CBCT image clearly showed a sclerotic appearance of both mandibular premolar regions (Fig. 5B). The patient's chest radiograph showed congenital ossification defects in both clavicles. Another observed skeletal deformity was spina bifida in the lower cervical spine and the upper thoracic spine (Fig. 6).
The patient began orthodontic treatment at 35 years of age. After orthodontic treatment, the impacted permanent teeth showed a progressive tendency to erupt in the coronal direction (Fig. 7), which seemed to be related to the extraction of deciduous teeth and orthodontic force applied with orthodontic buttons.
This case shows that in a CCD patient, tooth eruption did not occur without proper dental treatment, despite the passage of a 12-year period. Of particular note, in both the left and right posterior mandibles, the second primary molars were missing, and the eruption of both overlying second premolars was achieved without intentional dental treatment. It is unclear whether the loss of deciduous teeth was the cause or the result of tooth eruption. This case also showed that tooth eruption can be achieved with proper orthodontic treatment even in adult CCD patients.
Case 3
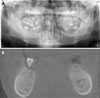
A 46-year-old woman visited our dental hospital in 2005 for the treatment of uncomfortable dentures. Panoramic radiography revealed multiple impacted permanent teeth and impacted supernumerary teeth (Fig. 8A). Another characteristic feature was a downward tilt of the right and left zygomatic arches. The skull views showed a thick skull cortex, underdevelopment of the maxilla, edge-to-edge bite, and Wormian bone in the cranial suture and anterior fontanelle (Figs. 8B and C). The chest radiograph showed underdevelopment of the right and left clavicles (Fig. 9).
After 13 years, the patient visited our dental hospital complaining of swollen gingiva around her upper left canine. A panoramic radiograph (Fig. 10A) showed multiple impacted permanent teeth and impacted supernumerary teeth similar to the finding in the image obtained 13 years prior. To obtain more detailed visual information to facilitate proper diagnosis, CBCT images were taken (Figs. 10B–D) and revealed multiple supernumerary teeth. The 5 supernumerary teeth were located in the areas of the right upper canine, left upper central incisor (with a dentigerous cyst), lower left first and second premolar, and lower right central incisor. Additionally, most of the supernumerary teeth displayed incomplete root formation. As in case 2, this case also supports the concept that tooth eruption does not occur without proper dental treatment, despite the passage of more than 10 years.
Discussion
Recent detailed clinical investigations have shown that CCD is a generalized skeletal dysplasia affecting not only the clavicles and the skull, but the entire skeleton. CCD is therefore considered to be a dysplasia rather than a dysostosis.9
Since early diagnosis of CCD is essential for initiating appropriate treatment, dentists should be aware of the characteristic features of CCD.4 CCD may present with a triad of features: multiple supernumerary teeth and delayed eruption of permanent teeth, partial or complete absence of the clavicles, and open sagittal sutures and fontanelles. This triad is pathognomonic for the diagnosis of CCD.10
This case report describes the clinical and radiographic manifestations of 3 CCD cases and investigates the eruption patterns of the patients' impacted permanent teeth. All 3 cases showed the delayed eruption of impacted permanent teeth, especially the anterior and premolar teeth. This delayed eruption is presumed to be related to the presence of incomplete cellular cementum or the reduced ability of periodontal ligament cells to induce osteoclastic differentiation.811
In case 1, a newly formed radiopaque mass was observed when the patient was around 9-10 years old. Since the visible dental signs of CCD, such as supernumerary teeth or eruption failure, are usually associated with the permanent dentition, and the hypoplastic midface usually becomes apparent only after the pubertal growth spurt of the mandible, the CCD of many patients is not recognized in their younger years.4 Since the mother in case 1 had CCD, she was able to recognize the mild features of the condition in her daughter. Therefore, the young patient started orthodontic treatment at the age of 8 years and quickly showed successful treatment outcomes of eruption patterns.
Case 2 involved a patient in whom several deciduous teeth were missing over a 12-year period, and some of his impacted permanent teeth showed eruption without orthodontic treatment.
Dense alveolar bone was apparent in the upper and lower premolar regions. This dense bone may have been related to a disturbance in bone resorption during normal tooth eruption.
Case 3 exhibited some impacted permanent teeth with no additional eruption over a 13-year period. The presence of 5 supernumerary teeth was confirmed by CBCT imaging. Supernumerary teeth could not be easily identified due to superimposition with adjacent structures on panoramic images. Delayed eruption could be explained by supernumerary teeth obstructing the eruption pathway, overlying dense alveolar bone, or other factors, such as the presence of incomplete cementum; however, these potential explanations have not been clearly supported.
The supernumerary teeth observed in CCD may result from the local abundance of odontogenic epithelium in periodontal tissues of developing as well as fully developed teeth.12 Supernumerary teeth can cause mechanical obstruction and may be the chief contributor to the impaction of permanent teeth observed in CCD. Other studies have suggested that the hyperdontia evident in cases of CCD may be regulated by environmental influences, along with epigenetic factors.13 Histological studies have shown that abnormal alveolar bone and cementum are associated with CCD.11 However, the presumption that cellular cementum is essential for tooth eruption was not supported by the findings of a similar study.7 Another suggestion is that the failure of the appropriate disintegration of Hertwig's epithelial root sheath can lead to the formation of gaps of the cemento-enamel junction, resulting in delayed eruption of permanent teeth.11 The periodontal ligament cells of CCD patients may express an impaired ability to support osteoclastogenesis, which may, in part, account for the delayed tooth eruption.8 It is unclear whether the prolonged retained deciduous teeth are another cause or a result of the delayed eruption of permanent teeth. Suggested factors for prolonged retained deciduous teeth are the lack of eruption potential and the lack of cellular cementum in the roots of permanent teeth.14
Early extraction of the primary teeth and the cutting of bony windows allows for permanent tooth eruption without orthodontic treatment. Another option is orthodontic treatment with surgical extraction. Normal tooth eruption occurred in the patients in cases 1 and 2 when those patients underwent proper orthodontic treatment. The sooner that patients with CCD can be diagnosed and initially treated, the higher the likelihood of better results.1
All 3 cases in this study displayed some common features: delayed eruption of permanent teeth, supernumerary teeth, underdevelopment of the maxilla, and clavicular hypoplasia. In case 2 in particular, parallelism of the mandibular ramus was apparent.15
Further studies are needed to better understand the cause of delayed eruption in CCD. According to this report, the causes of delayed permanent eruption were similar, yet certain aspects were different. For example, only case 2 showed characteristic dense alveolar bone. Some potential factors, such as the incomplete cementum layer of the unerupted teeth or the reduced ability of the periodontal ligament to induce osteoclastogenesis, may have contributed to delayed eruption in all 3 cases.





 XML Download
XML Download