

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Recurrent caries under restorations is the main reason for restorative failure and replacement in the primary dentition.12 Improper or delayed diagnosis of carious lesions may lead to significant loss of hard tissue and may result in unsuccessful treatment outcomes. A visual examination should be combined with a probing and radiographic examination to improve the detection of recurrent caries. Radiography is the most common and useful method for diagnosing recurrent caries under restorations, and bitewing radiography is usually preferred by clinicians.345 Despite being the most preferred radiographic technique, bitewing radiography has several drawbacks, such as distortion, superimposition, and poor beam angulation.6 Therefore, it may fail to provide adequate information regarding the diagnosis, location, and extension of recurrent caries under different restorations.7 Moreover, the radiopaque appearance of restorations may conceal the carious lesions.8 Cone-beam computed tomography (CBCT) was introduced in order to overcome the shortcomings of 2-dimensional radiographic techniques.9 CBCT enables the acquisition of 3-dimensional information regarding dentomaxillofacial structures in a single scan, including 180°-360° rotation around the structures using a coneshaped X-ray beam.10 Due to the high radiation exposure, CBCT must not be used routinely for the detection of caries, particularly among children. However, CBCT imaging can be conducted for various other reasons in children, such as evaluating impaction, eruption, and pathology.567891011 Therefore, available CBCT images taken for different reasons in children may also be used to diagnose recurrent caries during routine image interpretation.
Beam-hardening artifacts and streak artifacts are thought to be limiting factors in the detection of recurrent caries under restorations when assessing CBCT images.5 Beamhardening artifacts occur adjacent to high density structures and are seen as dark bands, and streak artifacts occur due to radiation from a metallic object and are seen as linear hyper-densities extending along the width of the field.12 The presence of beam-hardening artifacts and streak artifacts has the potential to completely affect the quality of the CBCT image and, thus, its diagnostic ability. The potential difference of an X-ray beam source, which is referred to as the tube voltage and is measured in peak kilovoltage (kVp), and the tube current, which is measured in milliamps (mA), are factors that may determine the quantity and quality of the X-ray beam.13 The tube voltage is thought to be the most important factor affecting image quality and diagnostic ability. High-contrast radiographs obtained with low tube voltage have been recommended for detecting caries using intraoral radiography.14 A previous study revealed that a tube voltage of 50 kVp was better than 65 kVp and 70 kVp when used with a phosphor-plate intraoral radiography system for detecting proximal caries in primary teeth.15 However, on the contrary, another study established that there was no significant difference between 60 kVp and 90 kVp for the diagnosis of artificial peri-implant defects and carious lesions in permanent teeth using intraoral radiography16. To the best of our knowledge, no studies have compared different CBCT setting parameters in detecting recurrent caries under amalgam restorations at the primary dentition.
In routine dental practice, exposure settings of CBCT systems are generally determined by manufacturer recommendations. Nearly all commercially available CBCT systems have pre-set exposure modes for different clinical needs and also allow for the manual selection of exposure settings. It is difficult to diagnose recurrent caries under amalgam restorations in primary teeth due to the compression of structures in intraoral radiography and the occurrence of metal artifacts in CBCT. Therefore, it is clinically useful to assess the performance of CBCT systems using different imaging settings for the visibility of recurrent caries lesions under restorative materials. The aim of this study was to assess the ex vivo diagnostic ability of 9 different CBCT settings in the detection of recurrent caries under amalgam restorations in primary teeth.
Materials and Methods
A total of 52 extracted or exfoliated primary mandibular first molars and second molars were included. Twenty-six teeth had dentine caries and 26 teeth did not have dentine caries. The presence of caries was determined by visual and intraoral radiographic examination prior to cavity preparation. Teeth were immersed in 2% sodium hypochlorite for 20 minutes and stored in distilled water. In all 52 teeth, Black class II cavities were prepared and then amalgam restorations were placed. In the 26 carious teeth, recurrent caries were left under amalgam restorations. The other 26 intact teeth that did not have caries but had been restored with amalgam restorations served as controls. Cavex Avalloy (Cavex Holland BV, Haarlem, Netherlands) was utilized with zinc phosphate liner for amalgam restorations (Adhesor Cement, SpofaDental, Jicin, Czech Republic). Each group of teeth was stained by a researcher with 2 different-colored nail varnishes. Teeth were randomly mixed prior to the acquisition of images to ensure random selection.
Image acquisition
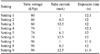
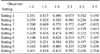
For the imaging procedures, teeth were placed in the mandibular molar sockets of a child mandible within a dry skull. The dry skull and the mandible were covered with 2 cm of red wax in order to simulate soft tissue. All teeth were randomly placed in the alveolar sockets together in groups of 4 (first and second mandibular deciduous molars on the left and right hemi-mandibles). After the teeth were placed, they were imaged using a 100×90-mm field of view (FOV), a 0.2-mm voxel size, and 9 different settings of a CBCT system (Planmeca ProMax 3D ProFace, Planmeca, Helsinki, Finland), as shown in Figure 1 andTable 1. No artifact reduction was used.
Image interpretation
Four observers, including 2 dentomaxillofacial radiology specialty students (observer 1 and observer 2) and 2 dentomaxillofacial radiology specialists (observer 3 and observer 4), separately reconstructed the multi-planar reformatted images in a dimly lit room. They used the software provided by the CBCT system (Planmeca Romexis, Planmeca, Helsinki, Finland) on a medical diagnostic monitor (NEC, Tokyo, Japan) that had a 21.3-inch screen and 2048×1536 resolution.12 The observers prepared panoramic and cross-sectional views with a 1-mm section interval and 1-mm thickness. A total of 10 images that were not included in the study were used for a calibration session prior to the interpretation sessions. No time restriction was placed on the observers, and evaluations of each image were repeated 1 week after the initial viewings.
For each tooth, the cross-sectional images were assessed for the presence or absence of recurrent caries under restorations and were scored using a 5-point scale as follows: 1, caries are definitely present; 2, caries are probably present; 3, uncertain or unable to tell if caries are present; 4, caries are probably not present; and 5, caries are definitely not present. Histological validation of the status of the caries was performed by serially sectioning each tooth mesiodistally in parallel to the long axis of the crown using an Accutom-50 (Struers, Ballerup, Denmark). Both sides of each section were examined under a stereomicroscope (×10) (Stemi 2000, Carl Zeiss, Jena, Germany). Teeth were recorded as either sound or having a carious lesion, which was defined as a demineralized white or yellowish-brown discolored area in the enamel or dentine. Histological status was determined by consensus of the researchers. Histological examination of the 52 tooth surfaces confirmed our first examination and revealed that 26 surfaces had dentine caries and 26 surfaces did not have caries.
Statistical analysis
Weighted kappa coefficients were calculated to assess the intraobserver and interobserver agreement for each setting. Kappa values were interpreted according to the following criteria: 0.10, no agreement; 0.11-0.40, poor agreement; 0.41-0.60, moderate agreement; 0.61-0.80, strong agreement; and 0.81-1.00, excellent agreement.17 Scores obtained for the different CBCT settings were compared with the gold standard using receiver operating characteristic (ROC) curves to evaluate the ability of observers to differentiate between teeth with recurrent caries and without recurrent caries. The area under the curve (AUC) values were calculated with standard errors and 95% confidence intervals, and AUC values for each setting were compared using the chi-square test and a significance level of α=.05. The effects of the observer, the reading, and the image setting on diagnosis were calculated using 3-way repeated analysis of variance (ANOVA). All calculations were carried out using Stata 12/MP4 statistical software (StataCorp LP., College Station, TX, USA).
Results
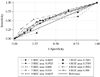
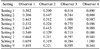
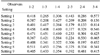
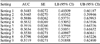
Table 2 shows the intraobserver kappa coefficients calculated for each observer for their first and second readings. The intraobserver kappa coefficients ranged from 0.366 to 0.664 for observer 1, from 0.311 to 0.447 for observer 2, from 0.597 to 1.000 for observer 3, and from 0.869 to 1 for observer 4. This suggested poor and moderate intraobserver agreement for observer 1 and observer 2, respectively, and strong and excellent intraobserver agreement for observer 3 and observer 4, respectively. Table 3 and Table 4 show the interobserver kappa coefficients for the first and second readings by the different CBCT imaging settings, respectively. Interobserver kappa coefficients among observers ranged from 0.133 to 0.814 for the first reading and from 0.197 to 0.805 for the second reading. In general, we found poor and moderate interobserver agreements for both readings. The AUC values for differ-ent settings for each observer and reading were also calculated. No statistically significant difference was found among different CBCT settings used for the detection of recurrent caries under amalgam restorations (P>.05). However, when the data were analyzed without taking into account intraobserver and interobserver dependency in general, the highest AUC values were found for setting 5 and setting 3, though they were not found to be statistically significant (P>.05) (Table 5). Figure 2 shows the ROC curves for observer 3 for the first reading of all settings. According to ANOVA, there was a significant main effect of observers (P<.05) and a non-significant main effect of reading and image setting on diagnosis (P>.05).
Discussion
The aim of this study was to evaluate different CBCT settings and determine the best setting for the detection of recurrent caries under amalgam restorations in primary teeth. No significant difference among various settings was found, despite setting 5 (78 kVp, 6.3 mA, and an average exposure time of 12.0 seconds) and setting 3 (60 kVp, 12.5 mA, and an average exposure time of 12.0 seconds) showing the highest AUC values. Our results suggested that variations in the tube current and the tube voltage did not affect the detection of recurrent caries under amalgam restorations. In addition, the low AUC values, most of which were lower than 0.60 for all observers, indicated that CBCT may not be the ideal imaging technique for the detection of recurrent caries in primary teeth. However, dentists are often asked to assess caries under amalgam restorations when CBCT images have been taken for other reasons, particularly among children, as amalgams are still preferred in most regions of the world. Potential limitations to the CBCT system should be taken into account when assessing recurrent caries under restorations. Furthermore, observer performance and diagnostic accuracy were not affected by using different CBCT settings through changing the tube voltage, tube current, or exposure time. Observer consistency increased with experience, as indicated by the contrast between observer 2, who was a new specialty student and had the lowest intraobserver and interobserver agreement values, and observer 4, who showed the highest intraobserver agreement values for all readings and was the most experienced specialist. Variations within and among observers were due to difficulties in interpreting the CBCT images for diagnosing recurrent caries. In a previous study, the highest AUC for images evaluated on a variety of display types was found for an image assessed on a medical diagnostic monitor that used dedicated software.12 Therefore, in this study, the same monitor and dedicated Planmeca software were used, which enabled the observers to scroll through images and easily inspect each section for caries or artifacts that resembled caries.
Dental caries are among one of the most common health problems. It is, therefore, crucial to assess available diagnostic methods in order to make an accurate and early diag-nosis.18 Detecting recurrent caries under amalgam restorations can be a complicated process when beam hardening artifacts mimic caries, or vice versa. Furthermore, detecting recurrent caries under restorations in primary teeth is of paramount importance, as they improve quicker than carious lesions in permanent teeth.19 Artificial carious lesions are easier to diagnose than real carious lesions. However, their appearance may not reflect actual clinical conditions. Therefore, we used real carious lesions under restorations that were clinically, radiographically, and histologically validated.
Despite the negative effect of metal artifacts on the quality and interpretability of CBCT images, a previous study found greater, yet statistically non-significant (P>.05) AUC values for CBCT images than for intraoral images in detecting recurrent buccal caries under restorations.5 In a study where the diagnostic abilities of visual inspection, film, charge-coupled device, photostimulable phosphor plate, and CBCT images were assessed in detecting proximal caries, experienced observers found higher AUC values for CBCT images, though the difference among the modalities was not statistically significant.20 The authors of the aforementioned study used images with a 0.3-mm voxel size, whereas we used a 0.2-mm voxel size, which may have improved our diagnostic ability. In addition, Kulczyk et al.21 examined the effects of the presence of amalgam fillings in detecting proximal caries and concluded that CBCT images should not be used as a diagnostic modality for detecting caries if amalgam fillings are present. That study included CBCT images of 102 extracted permanent teeth that were obtained with a 9-inch FOV, a 0.25-mm voxel size, an automatically adjusted tube current, a constant tube voltage of 110 kVp, and a 36-second scanning time, and, similar to our findings, showed that the presence of metallic artifacts made it difficult to detect recurrent caries in CBCT images. Although CBCT imaging provides a 3-dimensional visualization of recurrent caries, the presence of metallic artifacts from amalgam filling material represents a potential limitation to this imaging technique. Another predominant limitation of the CBCT system, motion artifacts, was not an issue in the ex vivo setting of our study.
To our knowledge, no previous study has compared the use of different CBCT setting parameters to detect recurrent caries under amalgam restorations at the primary dentition. However, a recent study assessed the effects of variations in tube current and FOV on the detection of a vertical root fracture in teeth with intracanal posts and found that decreasing the tube current resulted in a higher efficacy in detecting a vertical root fracture.22 According to another study, differences in exposure parameters did not affect the diagnostic ability of observers to detect a vertical root fracture.23
The main objective of our study was to evaluate the effects of changes in tube voltage and tube current settings on the detection of recurrent caries under amalgam restorations in primary teeth. We therefore did not attempt to reduce artifacts through settings offered by the CBCT system in order to keep our findings unbiased. Unlike intraoral images, CBCT images make it possible to view restorations and carious lesions in axial, coronal, and cross-sectional views. However, patients receive higher radiation doses with CBCT than with intraoral radiography, which must be taken into consideration. The average effective doses for a 10-year-old phantom and an adolescent phantom were found to be 116 microsieverts (µSv) and 79 µSv, respectively. It was also calculated that the percentage attributable lifetime mortality risks were 0.002% and 0.001% for a 10-year-old and an adolescent patient, respectively, which are considerably higher than the risk to an adult having received the same doses. It is, therefore, crucial that dental CBCT examinations on children must be fully justified over conventional techniques.24 Radiation exposure was not an issue in our ex vivo research. However, we used CBCT with a medium FOV and a 0.2-mm voxel size, as these settings are preferred for most diagnostic tasks. Ultimately, our findings may not apply to CBCT systems and images obtained using different settings.
In conclusion, there were no statistically significant differences among different CBCT settings used for the detection of recurrent caries under amalgam restorations in primary teeth. Our results suggest that variations in tube voltage and tube current did not affect the detection of recurrent caries under amalgam restorations in primary teeth.

 XML Download
XML Download