

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The advent of cone-beam computed tomography (CBCT) changed the patterns of imaging use in the field of dental and maxillofacial imaging. The field of view (FOV) and resolution obtained on most CBCT scanners provide a comprehensive depiction of critical anatomic structures in the maxillofacial region, extending into the calvarium and the neck. Hence, in addition to evaluation of any pathology associated with the hard tissues of the jaws and sino-nasal structures, the physiologic and pathologic calcifications associated with the soft tissues of the head and neck can be explicitly evaluated with CBCT. Vascular and intracranial calcifications are among the most studied soft tissue calcifications in the head and neck area.123 Pineal gland calcifications have been studied in both the medical and dental literature,245678 but these calcifications have largely been reported as incidental observations, with no specific clinical relevance.
The pineal gland is a neuronal structure located between the 2 cerebral hemispheres that produces melatonin, a hormone that modulates sleep patterns in both circadian and seasonal cycles.9 The pineal gland typically calcifies over time.910 Studies have shown that pineal gland calcification can be noted in children as young as 5 years.911 The degree and frequency of calcification have been noted to increase with age.10 Pineal gland calcification also depends on environmental factors, such as altitude and sunlight exposure.10 It has been hypothesized that increased pineal gland calcification results in decreased melatonin production.512
Reduced melatonin production has been implicated in a variety of neurodegenerative disorders such as migraine, stroke, schizophrenia, and Alzheimer disease.4571314 Patients referred for dental implant therapy usually tend to be individuals in their late 50s to early 60s, and therefore may be a vulnerable group for Alzheimer disease. To facilitate easy identification of the location of the gland and any associated calcification on CBCT scans, the pineal gland is usually noted as a midline calcification in the posterior cranial fossa in axial sections. The calcification is posterior and superior to the level of the sella turcica. As mentioned earlier, in a large-FOV CBCT scan, pineal calcification is usually an incidental finding. Hence, clinicians can contribute to the early diagnosis and prevention of challenging neurodegenerative conditions. Since most dental implant patients are middle-aged or older, the possibility of studying this phenomenon in these patients is ideal. The objective of this study was to analyze the CBCT scans of patients referred for dental implant therapy to evaluate the prevalence and extent of pineal gland calcification according to age and gender.
Materials and Methods
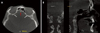
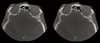
The present cross-sectional study consisted of the retrospective evaluation of CBCT scans of patients referred to the University of Connecticut School Of Dental Medicine for advanced imaging. An institutional review board (IRB) exemption was granted for this study by the University of Connecticut IRB. The inclusion criteria for the study were scans with a large FOV (170 mm×120 mm), which generally extended from the bregma (forehead) to the menton (lower tip of the bony chin) superoinferiorly and from the anterior nasal spine to the cervical spine anteroposteriorly, without any metallic or motion artifacts. The exclusion criteria were scans that did not adequately show the pineal gland area, had image artifacts that compromised the quality of the scans, or did not have associated details such as gender and age. All scans were acquired with a single CBCT machine (Accuitomo-170; J Morita Corp., Kyoto, Japan), and scans were obtained at 90 kVp and 10 mA. Initially, 1000 scans were screened on the basis of the inclusion and exclusion criteria, and ultimately, 500 scans were selected based on the inclusion criteria. The selected scans were de-identified by a research assistant to remove all patient identifiers. The investigator had access to the patients' age and gender from the Digital Imaging in Communications and Medicine data. The scans were imported and evaluated in a CBCT reconstruction program, Invivo5 (Anatomage Inc., San Jose, CA, USA). Pineal gland calcification was identified as a midline calcification in the posterior cranial fossa within the cranium (Fig. 1). Owing to its small size, pineal gland measurements were difficult in the coronal and sagittal planes. Hence, the size of the calcification was measured in the axial scans in the anteroposterior and lateral directions (linear measurements, Fig. 2). The area was calculated by marking the perimeter of the calcification (areal measurements, Fig. 2). The data were entered into Microsoft Excel (Microsoft Corp., Seattle, WA, USA). Statistical analysis was performed with SPSS version 17.0 (SPSS Inc., Chicago, IL, USA). Six weeks following the completion of the study, another investigator randomly reviewed 50 scans to investigate interobserver variation. A reliability analysis with interclass correlation coefficients was performed to assess interobserver variation. The data were analyzed using descriptive statistics to the calculate mean values and prevalence of pineal gland calcification. The difference between the prevalence among males and females was analyzed using the chi-square test. The correlations between the age of the patient and the linear and areal measurements of pineal calcifications were analyzed using the Pearson correlation coefficient.
Results
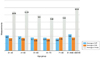
Of the 500 scans that were evaluated, 290 (58%) were from female patients and 210 (52%) were from male patients. Pineal gland calcification was noted in 294 scans, with a prevalence of 58.8%. Of these scans, 170 were from females (58.6%) and 124 were from males (59.0%). The chi-square statistic for the difference between male and female subjects was 0.0092 (P=.92). The difference was not statistically significant. The mean linear and areal measurements were higher in males than females (Fig. 3).
The patients ranged from 32 to 85 years of age, with a mean age of 63.42±10.43 years. The degree of calcification in different age groups is shown in Figure 4. The mean anteroposterior measurement was 3.73±1.63 mm, with a range of 1.14–8.55 mm. The mean lateral measurement was 3.47±1.31 mm, with a range of 0.88–8.01 mm. For each of the measures, the interclass correlation coefficient was measured, as well as the coefficient for linear measurements, which was 0.826 (0.604–0.923) for the anteroposterior measurements and 0.853 (0.667–0.935) for the mediolateral measurements. The mean area of calcification was 9.79±7.59 mm2, with a range of 1.20–55.87 mm2. For area, the interclass correlation coefficient was 0.986 (0.969–0.994). This basically means that the most consistent agreement was for the areal measurements and that there was good agreement for the anteroposterior and mediolateral measurements. There was no linear relationship between age and the measurements. In addition, there were no correlations between age and the areal or linear measurements (P=.454, r=0.232). However, it is interesting to note that all the measurements were high in patients 81 years of age and above. The difference in the average mediolateral dimension according to age was minimal.
Discussion
Pineal gland calcification, melatonin secretion, and their relationship to numerous neurodegenerative disorders have been a topic of interest to the medical community.1516 Although the prevalence of pineal calcification has been studied by many authors in the dental literature, few studies have investigated the correlations among age, gender, and the extent of pineal gland calcification.128 The present study evaluated the feasibility of CBCT for evaluating pineal gland calcification, and investigated its relationship to age and gender. The major limitation of this study is the lack of clinical and laboratory data on the function of the pineal gland, making it difficult to extrapolate these findings to neurodegenerative changes in a clinically relevant way.
As stated in the introduction, patterns of pineal gland calcification in younger individuals are different from those in older subjects.9 Pineal gland calcification may also depend on environmental factors, such as altitude and the amount of exposure to sunlight.11 In the current study, we did not observe any specific patterns of calcification. A possible explanation for this observation could be that none of our patients were younger than 31 years. Another clear limitation of this study is that a majority of our study population was from the northeast United States, which has sparse sunlight for several months each year.
The prevalence of pineal calcification in the present study was 58.8%. This prevalence is higher than has been reported in most previous studies using CBCT.12 Sedghizadeh et al.1 reported that the prevalence of intracranial physiologic calcifications in their study was 35.2%, and that 80% of cases were accounted for by pineal calcification. Barghan et al.2 reported a prevalence of 11.18% in their study. Studies of multi-slice CT have reported prevalence rates as high as 60%–80%, depending on the age group studied.11 In the dental literature, pineal calcification has been most often detected as an incidental finding, and has been disregarded as a physiologic process related to age.128 This is likely to be because many patients who receive care at dental clinics are ambulatory and are not often assessed for neurodegenerative disorders. With this study, the authors would like to emphasize that when such calcifications are present, it is important to obtain a thorough medical history from the patient and to assess any other signs and symptoms that might hint at a neurodegenerative pattern. While we do not suggest that every patient with pineal calcification will have a neurodegenerative disorder or should be referred for an evaluation of such conditions, it is nevertheless a consideration on the diagnostic list.
Males in general are known to have a higher degree of pineal calcification than females.610 In our study, the prevalence of calcification was slightly higher in female patients. However, this difference was not statistically significant. Many authors link such differences to the effect of melatonin on gonadotropins.61718 Melatonin antagonizes the effect of estrogen by stimulating the production of progesterone, while increased levels of testosterone cause a reduction in melatonin levels.61718 This is probably a reason why the role of melatonin has been extensively studied in the pathogenesis of endometrial carcinomas.18
The most important finding of the study was the absence of a correlation between gland calcification and the age of the patients. In addition, the average measurements did not vary significantly according to age. This may have been due to a lack of a sufficient sample size with calcifications in each age group. More than 200 patients who had calcifications were between 51 and 85 years of age. Since the size of the pineal gland varies across individuals, the degree of gland calcification has been suggested to be a more specific indicator of the gland's function.512 It has been shown that the degree of gland calcification is higher in patients with Alzheimer disease than in controls and patients with other types of dementia.5 Calcification has also been proposed to decrease the capability of the gland to produce melatonin.12 The uncalcified gland volume has been directly associated with the production of melatonin. This has been proven using magnetic resonance imaging, which is known to have better soft resolution than computed tomography.16 Melatonin receptors are found in a variety of tissues in the body, such as the retina, vasculature, immune system, skin, pancreas, and endometrium.17 Due to its effects on these tissues, melatonin has been implicated in neurodegenerative, malignant, and immunological disorders.17 Since melatonin exerts important functions in numerous tissues and is related to functional gland volume, it is important for studies to correlate the degree of gland calcification to melatonin production. As this study was a retrospective analysis, it did not address melatonin levels. Although the area of pineal calcification correlated positively with age in our study, this relationship was not statistically significant. It would be interesting to study the extent of calcification on CBCT and its correlation to the production of melatonin in a larger sample in future research in order to understand this correlation better.
The authors conclude that CBCT was helpful in detecting the presence of pineal gland calcification. The prevalence of pineal gland calcification was high as an incidental finding in patients undergoing implant therapy. Pineal gland calcification in males was more common than in females in the current study. However, the study did not show any correlations between age and linear measurements or the area of pineal gland calcification. Future research should focus on correlating melatonin production and the extent of calcification on CBCT in patients with clinical signs and symptoms of early neurological degeneration or deficits.

 XML Download
XML Download