

 PDF
PDF ePub
ePub Citation
Citation Print
Print


At the beginning of the 19th century, anesthetic procedures were introduced for more invasive dental procedures, such as surgery, endodontic treatments, and dental implants. The needles were thick and had to be sterilized, which was the reason why they constantly broke.1234 With the use of flexible and disposable needles, the chance of fractures has decreased, but they can still occur. There are multiple reasons for needle fractures in the mandibular branch: 1) a patient's (usually a child's) sudden movement at the moment of the nerve block;2567 2) an inexperienced professional performing the technique;6789 3) the use of pre-bent needles; and 4) manufacturing errors in the needle.
Any element apart from dental and bone structures found in the body is considered a foreign body.78 In general, they are asymptomatic, but can result in symptoms, depending on the location. In the case of a metallic foreign body such as an anesthetic needle, it is possible to observe it on regular radiographs, such as panoramic, side, and frontal teleradiographs. However, for the correct diagnosis, to ensure the proper localization of the object, and for optimal monitoring of the case, techniques specific for a given region should be used, such as computed tomography (CT).1610
Case Report
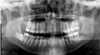
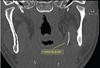
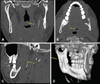
A 28-year-old male patient visited our dental office for exodontia of the third molars. During the inferior left alveolar nerve block, an anesthetic needle fracture occurred due to patient movement or a possible manufacturing error. The left mandibular third molar was removed and radiographic monitoring was carried out (Fig. 1). Initially, the authors opted to take a panoramic radiograph because it provides an image of both arches, including the areas of the jaw and soft tissues of the maxilla and mandible. The patient was monitored weekly with the goal of preventing painful symptoms. Panoramic radiographs obtained at intervals of 15 days demonstrated that the metallic object had changed its location. The patient did not complain of symptoms in that area (Fig. 2). To accurately localize the needle, the following radiographs were obtained: 1) panoramic, 2) lateral cephalography, and 3) multislice CT with 64 detectors (Figs. 3 and 4). It was found that the fractured needle was partially located in the medial pterygoid muscle and partially in the parapharyngeal space. Loss of the anatomical fat structure and the formation of granulomatous tissue was also observed (Figs. 5, 6, 7). The patient was referred to a head and neck surgery specialist for evaluation of the necessity of removing the object, but because of its location, monthly radiographic monitoring was chosen. Three months after the incident, the fractured fragment stabilized, obviating the need for surgical removal (Fig. 8). Quarterly radiographic monitoring was advised, and 2 years later, the patient did not present with any symptoms (Fig. 9).
Discussion
The occurrence of anesthetic needle fractures in dental practice is rare. However, their occurrence is frequently associated with the inferior alveolar nerve block, and the fragment usually settles in the region near the pterygomandibular raphe,14567810 as observed in this case. Therefore, complementary exams are necessary, as panoramic radiographs and specific radiographic techniques, including CT, are required to assess its location accurately.24567910 Some authors have reported the use of metal detectors, magnetic resonance imaging, and ultrasound for the accurate localization of the object.36710 In this case, panoramic radiographs, teleradiography, and the Waters view were performed to verify the location of the fractured fragment, as well as CT to evaluate its relationship with adjacent structures.
Bedrock et al. in 19992 described controversies regarding the removal of the fractured needle fragment, and argued that due to the absence of symptoms, the removal of the object is not generally necessary, as removal appears to be favorable only for the patient's psychological state with the goal of calming the patient. The possibility of migration of the fractured fragment is insignificant, although its removal might be recommended because of the possibility that it could cause injuries in adjacent tissues, especially when it is located near important structures.13610 In association with a needle fracture, the patient can present with an infection, inflammation, pain, trismus, difficulty in swallowing, and other symptoms indicating that surgical removal may be necessary.2389 In this case, fragment removal was initially recommended because of its migration in the first 3 months and the patient's uneasiness. After it stabilized, its location was verified to be in the parapharyngeal space (Fig. 5), the patient was reassured, and with the consensus of the team of professionals involved, it was decided to carry out radiographic monitoring of the fragment.
Dentists should develop the practice of explaining anesthetic block and possible complications during the procedure to their patients, requesting their cooperation in addition to a detailed inspection of the needle before the procedure. If defective needles are noticed, they should be discarded.123 It is very important that professionals know the proper technique for the nerve block of each nerve and use specific and appropriate needles, since the same type of needle should not be used for each nerve.234 This can prevent difficulties during dental local anesthesia.
It is necessary for dental surgeons to adopt procedures to prevent needle fractures and to perform a detailed inspection before anesthetic procedures. If a fracture occurs, it is ideal to inform the patient while trying to sedate him/her and to obtain the patient's cooperation in carrying out the necessary procedures for his/her well-being, such as radiographic monitoring or in some cases, surgery to remove the fragment.






 XML Download
XML Download