

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intoeing gait can occur due to metatarsus adductus, internal tibial torsion, and increased femoral anteversion angle (FAA). The first and second reasons are relatively easy to evaluate. Such intoeing gait spontaneously improves in most cases. If metatarsus adductus or internal tibial torsion does not spontaneously improve, a simple corrective device is usually required without intensive or surgical treatment [1]. However, FAA increase is hard to evaluate and its treatment is challenging.
FAA is defined as the angle between the transcondylar axis of the distal femur and long axis of the femur neck. FAA is around 30° at birth. Because of the common intrauterine position of hip external rotation, an infant appears to have more hip external rotation than internal rotation on physical examination. Soft tissue external hip rotation contracture will decrease over the first year of life and the increase of hip internal rotation from femoral anteversion will start to become apparent. FAA will gradually decrease from 30° to 40° at birth to 10° to 15° by early adolescence. Most of the improvement occurs before the age of 8 years. Therefore, cases with an 80% FAA increase do not require treatment [234]. However, if excessive FAA increase is not treated for cases that require treatments, tibial external rotation due to compensation at distal femur or pes planus may occur. The clinical state of such cases may be confused by the external appearance of intoeing gait improvement while the lower limb deformity is actually aggravated. In addition, such a case might significantly increase the frequency of lower limb symptoms like knee pain when patients reach adulthood [5]. Symptomatic intoeing gait is commonly treated by having children wear gait plates, shoes, and orthotic devices, although the supporting evidence for these strategies is weak [36]. Surgery is necessary for some of these cases [5]. Persistent and severe tibial medial or lateral torsion after 8 years of age with medial torsion beyond 15° and lateral torsion beyond 30° may be corrected by supramalleolar tibial rotational osteotomy. Severe femoral antetorsion exceeding 50° after 8 years of age might also need surgical correction. For surgical correction, medial rotation should exceed 85° while lateral rotation should be <10° [7]. Therefore, it is important to decide whether observation with follow-up is sufficient or whether further treatment is required for patients with increased FAA. To decide the proper treatment, knowledge about the precise normal FAA according to age and gender as well as natural course of FAA change in children with intoeing gait might be important [7]. Although there are studies about FAA of normal adults and patients with cerebral palsy [8910], no studies have reported FAA of normal children in Korea.
FAA can be evaluated by physical examination, simple X-ray, ultrasonography, computed tomography (CT) scan, nuclear magnetic resonance, and fluoroscopy [11]. Physical examination and simple X-ray have shown low accuracy and reliability [1213]. In addition, they have challenging methodological problems due to difficulties in maintaining position of children for practical use. It has been reported that physical examination results are significantly correlated with tibial and femoral torsion angles by CT scan for children with intoeing gait [1415]. However, both physical examination and CT scan have low accuracy. In contrast, three-dimensional computed tomography (3D-CT) reconstruction, which has been used in diagnosis of a wide range of diseases, has higher accuracy and reliability for measuring cadaveric skeletal FAA compared to CT measurement [16171819]. In addition, improvements in processing software and 3D-CT reconstruction technology have resulted in high intra-observer and inter-observer reliability of 3D-CT for FAA measurement of patients with cerebral palsy regardless of femoral neck-shaft angle or postural deformity [20], proving the usefulness of 3D-CT for FAA measurement. Recently, the 3D-CT method for measuring the FAA has shown high intra-rater and inter-rater reliabilities [21]. It can be considered for use in children with intoeing gait for comparison with normal young children. Although other methods, such as fluoroscopy, ultrasonography, and magnetic resonance imaging, have been attempted in the measurement of FAA [22], their reliability and utility have not been proven. In addition, their complex processes have lowered their usability for FAA measurement.
Thus, the objective of this study was to measure FAA using 3D-CT reconstruction image for children with intoeing gait. Initial and follow-up images taken at least 1 year later were used to observe FAA changes with time. First, FAA changes were analyzed depending on age, gender, and initial FAA when aggressive treatment was not performed in children with intoeing gait. Second, the relationship between initial FAA and FAA change based on FAA at birth was examined.
MATERIALS AND METHODS
Subjects
A total of 200 limbs of 100 children who visited our foot clinic with symptomatic intoeing gait as the main complaint with initial and follow-up (at least 1 year) 3D-CT images from January 2006 to December 2016 were retrospectively reviewed. Children with intoeing gait suspected to have increased FAA clinically were selected. Diagnosis of intoeing gait was simply made by visual gait analysis if there was >5° of internal rotation on both legs in the clinic. Children were chosen if their knees and patella were turned inward while gaiting. Subjects who showed abnormal gait due to orthopedic problems such as injury to lower limbs were excluded. Those who showed abnormal gait without developmental disorders were included in this study. Children with limited range of motion were also excluded. Family history of rotational problems was taken. Information of developmental history and the nature of disability, such as tripping or falling, was also taken. Whether the child preferred to sit on the floor in a ‘W-sitting’ or reversed tailor position was also investigated. However, quantitative gait analysis such as 3D motion analysis was not performed.
Children who underwent observation with simple posture correction, such as tailor position and stretching exercise for Achilles tendon, and hamstring without more active treatments, such as corrective device or surgery, were included for analysis. Since caregivers of children wanted to periodically observe changes through examination rather than active treatment, changes of intoeing gait were measured with 3D-CT at intervals of more than 1 year. It has been reported that intoeing gait due to excessive FAA will increase at 4 to 6 years of age and then gradually decrease at 13 to 14 years of age [2]. Therefore, the subjects of this study were divided into three groups according to their age at the initial 3D-CT examination: group 1 (≥4 and <6 years), group 2 (≥6 and <8 years), and group 3 (≥8 and <10 years). Assuming that FAA was 30° at birth, correlation between initial FAA and FAA change were determined in this study.
Radiologic evaluations using 3D-CT
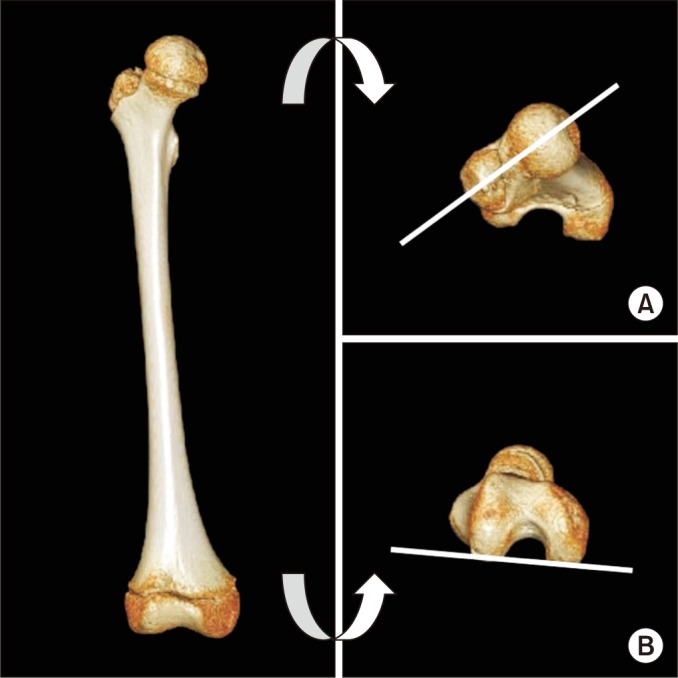
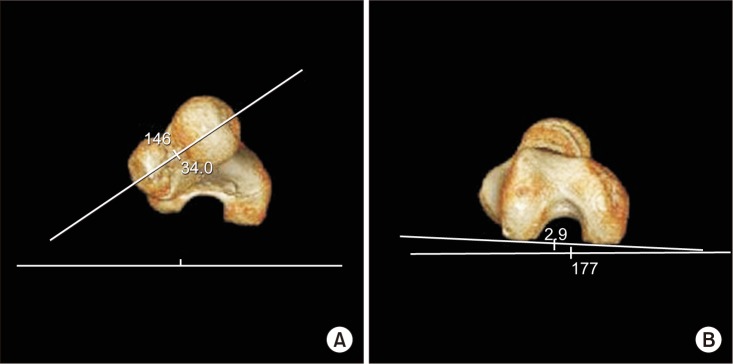
For CT scans, children were positioned supine with the direction of sliding side of the table to be caudal using a 64-channel CT scanner (Brilliance 64; Philips Medical Systems, Best, the Netherlands). Both knees were fully extended. Both limbs were fixed with strap on the table to prevent any movement. CT imaging of the bilateral femur was done. Image acquisition parameters were: field of view=314 mm; detector collimation=64×0.625 mm; table movement speed=44.4 mm/rotation; gantry rotation speed=1 second; kVp=120; and mAs/slice=36. The image was remodeled with thickness of 2 mm and spacing of 1 mm. Extended Brilliance Workspace ver. 2.0 software (Philips Medical Systems) was used to reconstruct 3D images using the volume rendering method. Corresponding images were acquired after 3D-CT reconstruction (Fig. 1). From the image obtained, FAA was measured by one doctor from the Department of Rehabilitation Medicine. Femur neck angle was calculated through the measurement of neck axis of femur against the horizontal axis. The neck axis of femur was used as reference axis for proximal. It was set as the line intersecting two center points of the neck of femur and the head of femur craniocaudally. To calculate the condylar angle, the angle of medial and lateral condylar axis against the horizontal axis was measured. Similarly, the medial and lateral condylar axis was used as the reference axis for distal. It was set as the line encountering the most posterior aspects of medial and lateral condyles of distal femur from the caudocranial of the 3D image (Fig. 2). FAA was then measured by subtracting the condylar angle from the femur neck angle if they were in the same direction against the horizontal axis or by adding the two angles if they were in the opposite direction [21].
Data analysis
Initial FAA was compared among the three age groups. Difference between the initial FAA and follow-up FAA was calculated. FAA changes according to age, gender, and initial FAA were analyzed.
Statistical processing
Data was processed statistically using SPSS version 21.0 for Windows (IBM SPSS, Armonk, NY, USA). Comparisons were statistically analyzed using one way analysis of variance (ANOVA) followed by Tukey's post-hoc test, independent t-test, and paired t-test. Statistical significance was set at p<0.05. Correlations of FAA change with age, gender, initial FAA were analyzed using Pearson correlation coefficient.
RESULTS
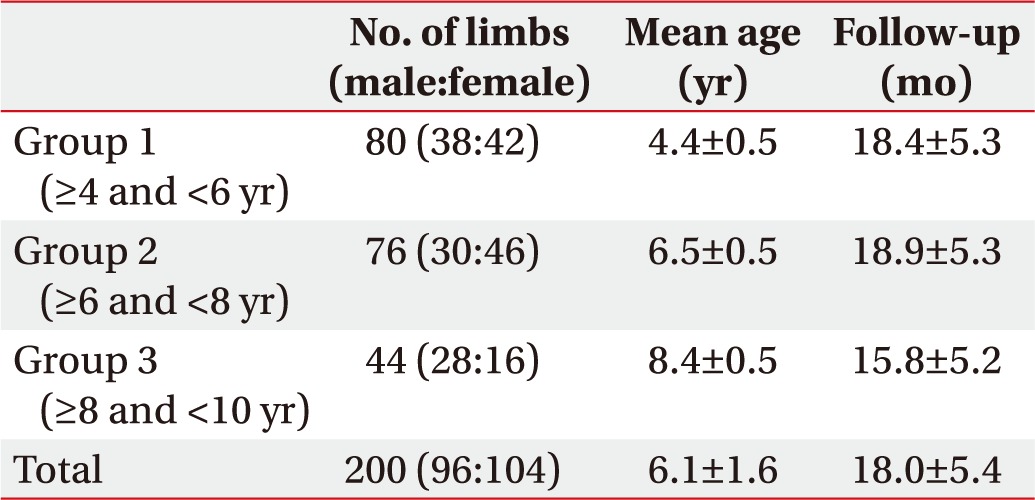
Among a total of 200 limbs of 100 patients, 96 limbs were from male patients (n=48) with a mean age of 6.1±1.6 years. Their average period from initial FAA to follow-up 3D-CT was 18.0±5.4 months. Group 1 consisted of 38 limbs from males and 42 limbs from females with a mean age of 4.4±0.5 years. Their average period from initial FAA to follow-up 3D-CT was 18.4±5.3 months. Group 2 had 30 limbs from males and 46 limbs from females with a mean age of 6.5±0.5 years. Group 3 was composed of 28 limbs from males and 16 limbs from females with a mean age of 8.4±0.5 years. Average periods from initial FAA to 3D-CT in groups 2 and 3 were 18.9±5.3 months and 15.8±5.2 months, respectively (Table 1).
Change of FAA according to age groups
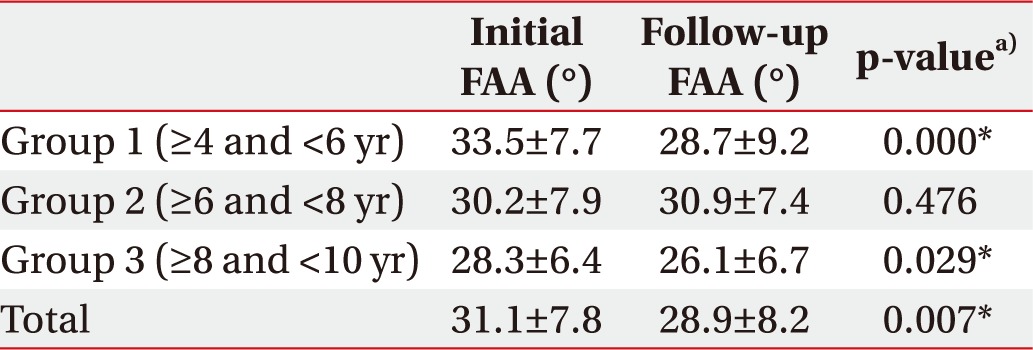
The initial FAA of group 1 was measured at 33.5°±7.7°. Follow-up FAA of group 1 was significantly reduced to 28.7°±9.2° (p=0.000). The initial FAA of group 2 was 30.2°±7.9°. Follow-up FAA of group 2 was increased to 30.9°±7.4°. However, the increase was not statistically significant (p=0.476). The initial FAA of group 3 was 28.3°±6.4°. It was decreased (p=0.029) to 26.1°±6.7° at follow-up. The average initial FAA of all subjects was 31.1°±7.8°. The mean follow-up FAA for all subjects was significantly (p=0.007) decreased to 28.9°±8.2° (Table 2).
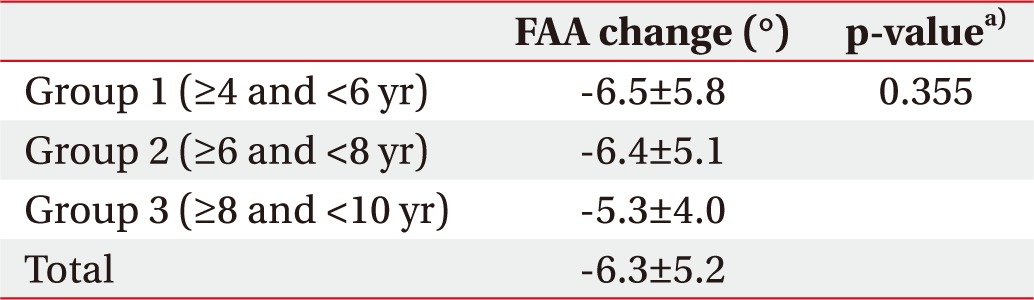
FAA changes in groups 1, 2, and 3 were −6.5°±5.8°, −6.4°±5.1°, and −5.3°±4.0°, respectively. Differences in FAA changes among the three groups were not statistically significant (p=0.355) (Table 3).
Factors affecting FAA change
Gender and FAA change
The mean age of 96 limbs of 48 male children was 6.3±1.7 years. Their initial FAA and follow-up FAA were 31.8°±7.2° and 29.3°±7.7°, respectively. The mean age of 104 limbs of 52 female children was 5.9±1.5 years. Their initial FAA and follow-up FAA were 30.4°±8.2° and 28.6°±8.2°, respectively.
Initial FAAs of male and female children were not significantly (p=0.200) different from each other. Follow-up FAAs of male and female children were not significantly (p=0.213) different from each other either. However, FAA decrease from initial to follow-up was significantly (p=0.012) more in female children than that in male children (Table 4).
Correlation between age and FAA change
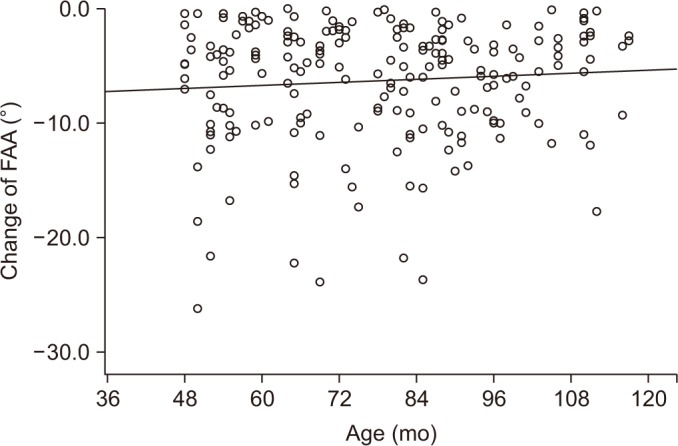
When FAA changes were compared according to age at initial 3D-CT imaging, FAA change was not significantly greater when the initial age was younger (Pearson correlation=0.083, p=0.243) (Fig. 3).
Correlation between initial FAA and FAA change
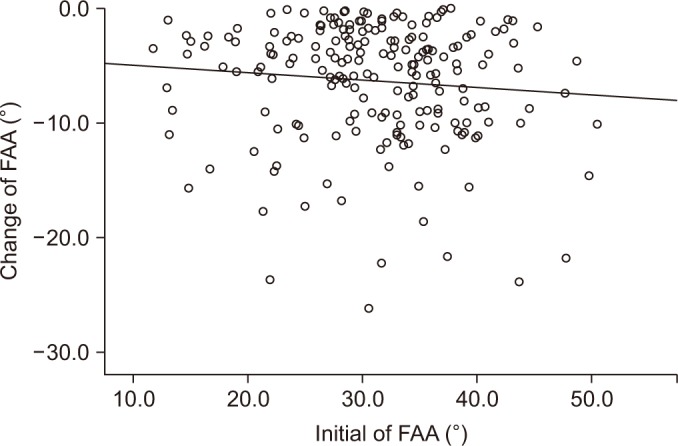
FAA change was significantly greater when initial FAA was larger (Pearson correlation=−0.096, p=0.018) (Fig. 4). When children were divided into two groups (initial FAA <30° or ≥30°), the group with initial FAA ≥30° showed significantly (p=0.019) more FAA change (−6.8°±5.4°) compared to the group with initial FAA <30° (FAA change of −5.6°±4.9°) (Table 5).
DISCUSSION
Fabry et al. [4] performed FAA studies using 316 limbs from 175 children with intoeing gait. Their average initial FAA was 42.68°±6.7°. In that study, 154 limbs in 77 children were re-evaluated after an average follow-up time of 5 years 6 months, ranging from 1 year to 18 years 5 months. The average follow-up FAA in that study was 39.48°±7.2°. They reported that FAA was decreased before 8 years of age. However, there was no significant change in FAA after 8 years of age [4]. Since most studies have been performed by plain radiography, which has low accuracy and reliability for examination, accurate angle measurement might not have been achieved in those studies. No prior studies have reported FAA changes using 3D-CT image.
Our study results using 3D-CT showed that follow-up (at least 1 year) FAA in children with intoeing gait was decreased at the age of 4–6 years and 8–10 years. The initial FAA was the greatest at age of 4–6 years among the three age groups. This age group also showed the greatest FAA decrease at follow-up. This is partially consistent with results of a previous study [14]. However, the average FAA of children 6–8 years of age was increased at follow-up. Such a difference might be due to different lifestyles between Korea and Western countries. The present study on Korea children did not show spontaneous improvement since children had a more sedentary lifestyle compared to children in Western countries. In addition, relatively more children habituate ‘W-sitting’ during sedentary lives in Korea. Children in Korea usually enter elementary school around the age of 6–7 years. Children have to sit in chairs for a long time with increasing school grades. This might have resulted in the decreased FAA for children at 8–10 years of age observed in this study. Further study about normal FAA according to age with normal Korean children may help elucidate the natural course of FAA change.
Follow-up FAA was significantly decreased in groups 1 and 3. However, follow-up FAA in group 2 was increased, although the increase was not statistically significant. The difference might be due to various characteristics of subjects since this study reviewed medical records of children who visited a foot clinic due to notable or at least visible intoeing gait. In addition, the follow-up period might not be enough to reveal significant change in FAA for those in group 2. If insignificant FAA change was due to notable intoeing gait, this may imply that children with intoeing gait who have severely increased FAA need to consider active treatment at early ages. Future study with longer follow-up period is required to verify other significant FAA changes and to confirm whether FAA changes shown in this study might be due to a relatively short follow-up.
There was a negative change in FAA in group 2. Their FAA at the follow-up were unusually increased. However, the mean values of initial and follow-up FAA for all children were almost unchanged because FAA values of some of these group 2 children were outliers. Most children showed decreased FAA at follow-up.
The average FAA was decreased in both male and female subjects, although female subjects showed more of a decrease in FAA (−7.1°±6.1°) than male subjects (−5.3°±3.9°). The difference in FAA change was statistically significant between male and female subjects, although their follow-up FAA values were not significantly different. This result may be construed as different tendency of FAA change according to gender. Therefore, further study with increased number of male and female subjects is needed to clearly explain such differences.
The FAA change was greater when the age at initial 3D-CT imaging was younger. However, such difference was not statistically significant. The FAA change was significantly greater when the initial FAA was greater. This might be due to the possibility that younger children have more chance to change FAA spontaneously with development. It might also be due to the effect of more participation in conservative treatment, namely simple posture correction and stretching exercise, due to their relatively severe intoeing gait. Therefore, future study on normal FAA in Korean children with treatment protocol is needed to determine the effect of conservative treatment such as simple posture correction on FAA change. In addition, conservative treatment such as simple posture correction and stretching exercise might not be as effective for older children with intoeing gait and smaller initial FAA compared to that for younger children with higher initial FAA. These children should be followed up with more clinical caution.
The present results showed that FAA at follow-up of more than a year in children with intoeing gait was decreased and their abnormal gait was improved. Thus, in children with intoeing gait, careful observation without any active treatment might be sufficient due to the natural course of FAA which will decreases with age.
We acknowledge that this study has certain limitations. First, the follow-up period was short (about 1 year) and no significant conclusion could be drawn. Therefore, longer follow-up (more than 3 years) is necessary to confirm FAA changes in children with intoeing gait. Second, we did not evaluate difference in FAA between normal children and children with intoeing gait. Thus, further study is needed to determine FAA changes according to age and sex in normal children. Third, the age of subjects was limited to 4 to 10 years old in this study. We divided these patients into three groups and measured changes in FAA. However, it is necessary to measure changes in FAA in children of all ages to define the standard FAA of children. Finally, we did not analyze FAA difference between male and females by age in each group. Therefore, future large scale study is needed to analyze such differences.
The 3D-CT method for measuring FAA has been proven to have high intra-rater and inter-rater reliabilities [21]. To the best of our knowledge, this is the first study that evaluates FAA changes according to age, gender, and initial FAA using 3D-CT in children with intoeing gait. Despite several limitations, results of this study provide valuable information on FAA change in children with intoeing gait.
In conclusion, using 3D-CT images of children with intoeing gait, the greatest initial FAA was found in children at age of 4–6 years among the three age groups. Their FAAs were significantly decreased when this age group was followed up for an average of 18 months. FAA was decreased significantly more in female subjects compared to that in male subjects. In addition, children with younger age at initial 3D-CT imaging and those with greater initial FAA showed more FAA decrease at follow-up.


 XML Download
XML Download