

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cardiac autonomic dysfunction is commonly associated with cardiovascular disease, and it has been reported in subjects with risk factors for developing cardiovascular disease. Autonomic dysfunction in these populations is mainly characterized by an increase in sympathetic activity and withdrawal of parasympathetic activity. This autonomic imbalance increases cardiac load and ventricular instability, leading to an increased risk for the progression of heart disease and worse clinical outcomes [1]. Post-exercise heart rate recovery (HRR) provides a noninvasive and clinically feasible method to quantitatively assess parasympathetic function [2].
Several studies have shown that impaired HRR after exercise cessation is associated with poor clinical outcomes, including an increased risk of mortality in subjects referred for stress testing [23456789101112]. Youn et al. [11] showed that impaired post-exercise HRR independently predicts clinical outcomes in prospectively and consecutively enrolled acute decompensated heart failure patients. Some studies have reported an association of HRR with peak oxygen consumption (VO2max) [913]. VO2max during a cardiopulmonary exercise test (CPET) is a powerful independent prognostic marker to risk stratify patients with heart disease, and it is also an objective measure of functional capacity [141516]. Based on these reports, we hypothesized that HRR might also be related to the degree of increase in cardiopulmonary exercise capacity. However, few studies have examined whether HRR is correlated with increased cardiopulmonary exercise capacity expressed as the changing ratios of VO2max and maximal metabolic equivalents (METmax) in populations with acute myocardial infarction (AMI).
Thus, the objective of this study was to determine if the HRR in the first exercise tolerance test (ETT) performed 3 weeks after AMI onset can predict not only the clinical outcomes but also the degree of improvement in functional capacity in patients with AMI.
MATERIALS AND METHODS
This retrospective study analyzed the medical records of 655 patients diagnosed with AMI (ST elevation and non-ST elevation myocardial infarction) between August 2014 and July 2016 who were referred to our rehabilitation center after undergoing percutaneous coronary intervention (PCI). Among the patients who underwent ETT at about 3 weeks after the onset of myocardial infarction (T0) and about 3 months after the completion of the first ETT (T1), the following were excluded: (1) those with an unstable medical condition, such as a recurrence or re-admission during cardiac rehabilitation, those who underwent cardiac surgery, and those with unstable musculoskeletal conditions such as severe pain, contracture, and paralysis; (2) those with high risk factors on risk classification (i.e., left ventricular ejection fraction [EF] <40%); and (3) those who participated in a center-based cardiac rehabilitation program. Ultimately, 60 patients (53 men, seven women) were included in this study.
This study was approved by the Chonnam National University Hospital Institutional Review Board (No. CNUH-2017-031).
All patients were educated regarding the importance of the modification of risk factors and regular exercise at about 3 weeks and 3 months after the AMI onset. However, patients who participated in center-based cardiac rehabilitation programs were excluded because such patients exhibit a significant improvement in functional capacity due to exercise training, and this could introduce a confounding variable. All included patients performed a symptom-limited ETT using the Modified Bruce Protocol.
Study outcomes were estimated from the ETT at both aforementioned assessment points. The body mass index (BMI) and history of comorbid conditions were assessed prior to the ETT. Heart rate (HR), VO2, and METs recorded at baseline and during ETT using an integrated metabolic measurement system (TrueOne 2400 Metabolic System; Parvo-Medics, Sandy, UT, USA) were used as clinical variables. Resting HR (HRrest), maximal HR (HRmax), resting systolic blood pressure (SBPrest), resting diastolic blood pressure (DBPrest), maximal SBP (SBPmax), and maximal DBP (DBPmax) were estimated using an automatic blood pressure and a pulse monitor, and a subjective measure of the rate of the perceived exertion was recorded. Changing ratios of VO2max and METmax were calculated by subtracting VO2max and METmax obtained at T0 from those obtained at T1, dividing it by the VO2max at T0, and multiplying by 100.
After achieving a peak workload, the treadmill slowed down the slope and speed for 5 minutes and then stopped. The patients recovered in a comfortable and relaxed seated position after a ‘cool down’ period. HRR was defined as the difference from HRmax to the HR measured at specific time intervals – immediately after the cool down period (HRR-0) and 3 minutes after the completion of ETT (HRR-3).
Data were statistically analyzed with IBM SPSS Statistics ver. 22.0 (IBM, Armonk, NY, USA). We used a paired t-test to compare the categorical variables. The Pearson correlation coefficient and multivariate regression analysis were used to establish a link between the changes in the ratio of functional capacity and HRR. For the statistical tests, a p-value <0.05 was considered to be significant.
RESULTS
General characteristics of subjects
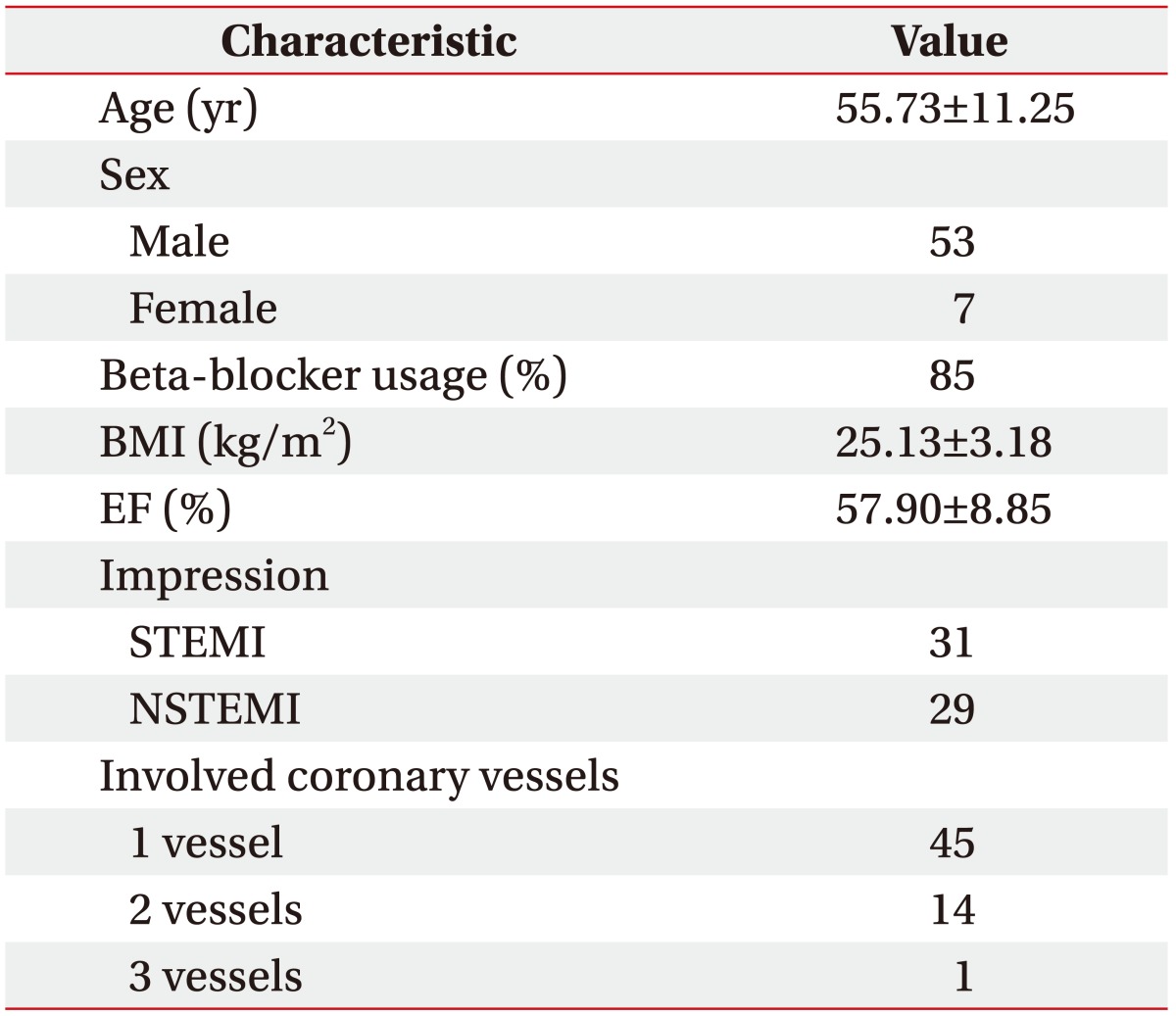
The subjects' general characteristics, including age, sex, beta-blocker usage, BMI, ejection fraction, and impression, are shown in Table 1. The mean participant age was 55.73 years. The patients were predominantly male, and 85% of the included patients were receiving beta-blockers. The average ejection fraction was 57.90%±8.85%. The ratio of ST elevation and non-ST elevation myocardial infarction was also similar.
Variables at 3 weeks after AMI onset and 3 months after first ETT
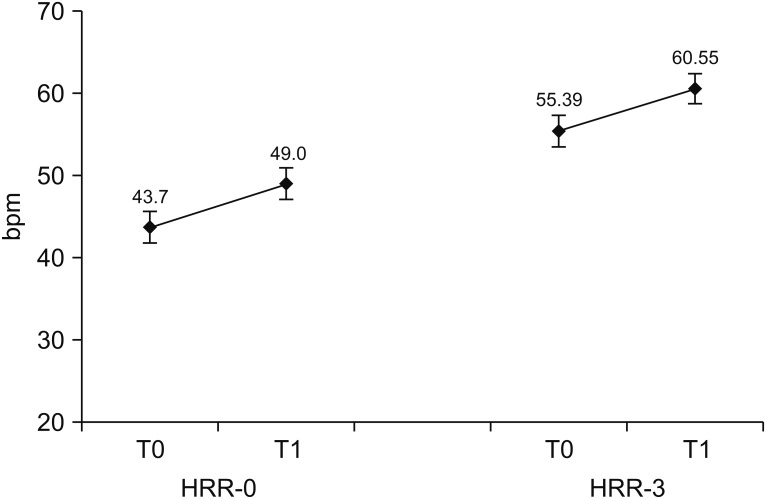
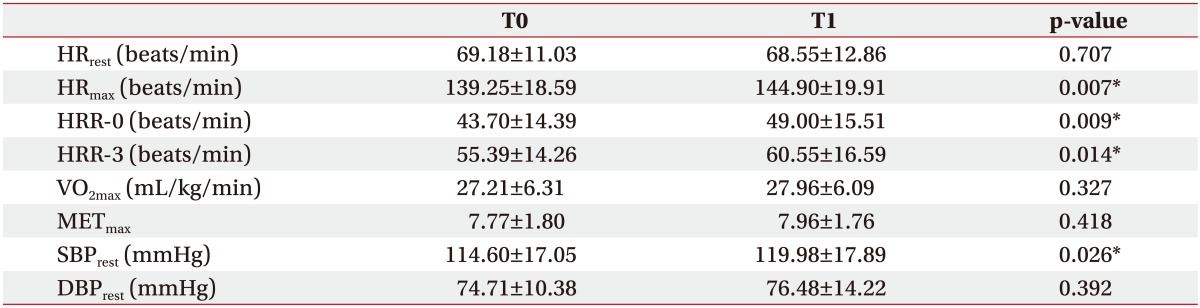
Post-exercise HRR-0 was a mean 43.70±14.39 at baseline and 49.00±15.51 after 3 months. Post-exercise HRR-3 was 55.39±14.26 at baseline and 60.55±16.59 after 3 months (Fig. 1). HRR-0 and HRR-3 improved significantly over time (p=0.009, p=0.014). The VO2max was 27.21±6.31 mL/kg/min at baseline and 27.96±6.09 mL/kg/min after 3 months. The METmax was 7.77±1.80 at baseline and 7.96±1.76 after 3 months. There was no significant change in cardiopulmonary exercise capacity (VO2max and METmax) over time (p=0.327, p=0.418) (Table 2).
Correlation between HRR and cardiopulmonary exercise capacity
We performed a Pearson's coefficient correlation to determine whether the HRR at T0 and T1 is associated with cardiopulmonary exercise capacity in each test.
HRR-0 at T0 was associated with VO2max at T0, and this relevance was statistically significant (r=0.469, p<0.001). Similar results were seen for METmax (r=0.469, p<0.001). HRR-3 at T0 was significantly correlated with VO2max at T0 (r=0.392, p=0.002). HRR-0 at T0 was significantly associated with VO2max at T1 (r=0.396, p=0.002). Likewise, similar results were seen for METmax (r=0.365, p=0.004). There was a significant correlation between HRR-3 at T0 and VO2max at T1 (r=0.289, p=0.027).
There were significant relationships between HRR at T1 and cardiopulmonary exercise capacity at T1 (Table 3).
Correlation between HRR at T0 and changing cardiopulmonary exercise capacity ratio
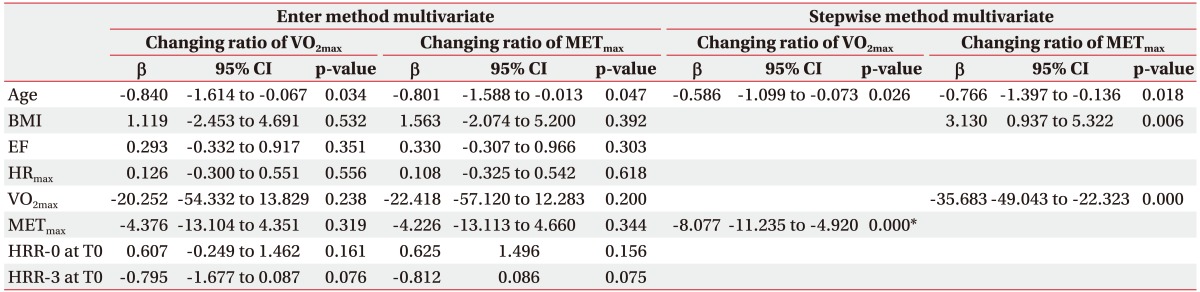
Both HRR-0 and HRR-3 at T0 were not correlated with the changing ratio of VO2max (r=-0.091, p=0.491 and r=-0.117, p=0.377, respectively). Neither HRR-0 nor HRR-3 at T0 was correlated with the changing ratio of METmax (r=0.168, p=0.199 and r=-0.186, p=0.159, respectively) (Table 4). These results were similar in a multivariate regression analysis. In the multivariate regression analysis, both HRR-0 and HRR-3 at T0 did not show independent prognostic value for the changing ratio of cardiopulmonary exercise capacity when controlled for age, BMI, EF, HRmax, VO2max, METmax. The stepwise method multivariate regression analysis also did not indicate an independent association of both HRR-0 and HRR-3 with the changing ratio of cardiopulmonary exercise capacity after adjusting the variables mentioned above (Table 5).
DISCUSSION
Here we attempted to elucidate the relationship between functional capacity and autonomic function. A significant association has been reported between HRR and peak VO2 to date. Sheppard et al. [9] reported that HRR after a cardiopulmonary exercise test was correlated with peak VO2 in patients with heart failure. Bilsel et al. [13] demonstrated that patients with an abnormal HRR had a lower VO2max value than those with a normal HRR. Similarly to other studies, this study demonstrated that HRR is correlated with cardiopulmonary exercise capacity. Unlike other studies, this study showed that HRR at T0 is also significantly related with cardiopulmonary exercise capacity at T1. In other words, subjects with a lower baseline HRR would have lower functional capacity, even after a few months.
The main purpose of this study was to determine the relationship between autonomic function and changes in functional capacity in patients with AMI. We hypothesized that there would be a relationship between the two. The study showed a significant relationship between HRR at T0 and exercise capacity at T0 as well as between HRR at T0 and exercise capacity at T1, but not between HRR at T0 and a changing ratio in functional capacity. Therefore, these findings may be interpreted as reflecting the initial severity rather than the direct impact of the changes in exercise capacity.
Youn et al. [11] reported that Post-exercise HRR is an index of autonomic function associated with clinical outcomes in patients with heart disease, and the increase in HRR represents a positive adaptation of autonomic function. This study showed that the autonomic response can improve over time. However, increases in exercise capacity were not significant. That is, the passage of time did not increase cardiopulmonary exercise capacity on its own without intervention, such as with exercise-based cardiac rehabilitation. Several studies have shown that cardiac rehabilitation improves physical health and exercise capacity in patients with coronary heart disease [171819]. Therefore, another noteworthy point in our study is that interventions such as exercise-based cardiac rehabilitation may be necessary to improve cardiopulmonary exercise capacity.
We attempted to clarify whether a change in exercise capacity after a few months can be predicted in relation to autonomic dysfunction upon onset of AMI. Unfortunately, we have not proven the hypothesis we established in this study. However, it is meaningful that we reported the relationship between HRR at initial ETT and exercise capacity after three months after first ETT, unlike other studies that have reported the relationship between HRR and exercise capacity only at one time point. In addition, this study is significant in that it clarified the change over time of autonomic dysfunction after AMI. There was a previous study of autonomic function improvement by active center-based cardiac rehabilitation, but few studies have investigated the natural course of autonomic function [20].
Our study has some limitations. First, it was retrospective, so the results may have been affected by its observational nature. The potential for referral bias exists because this report selected data from an exercise test database. However, to reduce as much intervention bias as possible, this study excluded patients who underwent a center-based cardiac rehabilitation program to enable an investigation of the natural course on the relationship between HRR and cardiopulmonary exercise capacity. However, it should be noted in interpreting this result that although this study targeted patients who did not participate in a center-based cardiac rehabilitation program, patient education was performed in the same way at every visit. Second, the sample size was small due to the cost of follow-up ETT, patients' lack of motivation, and patients' difficult hospital accessibility. Third, other factors such as beta-blocker use may have influenced autonomic function, and we did not consider such factors in our analysis. However, studies have demonstrated that beta-blockers were not associated with post-exercise HRR and did not modify the association between HRR and clinical outcomes [2911]. Finally, since the exercise intensity, time, frequency, and duration of each patient was uncontrolled, there might be a difference in the degree of adaptation of autonomic function according to exercise amount. Future studies including formalized cardiac rehabilitation protocols are desirable.
In conclusion, this study shows that post-exercise HRR is associated with functional capacity as well as clinical outcomes. However, this measurement could not establish the prognostic value in relation to the degree of cardiopulmonary exercise capacity enhancement.


 XML Download
XML Download