

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Congenital muscular torticollis (CMT) is one of the most frequent musculoskeletal disorders among children, with prevalence rates ranging from 0.3% to 3.92% [12]. CMT might be defined as a developmental disorder of the sternocleidomastoid muscle (SCM) that is characterized by fibrosis, eventually leading to shortening of the SCM and resulting in limited neck motion [34].
About 90% of CMT cases can be cured with stretching exercises only, without musculoskeletal complications [1]. However, about 10% of CMT cases hardly respond to stretching exercises. Surgical release is needed for this severe subgroup of CMT to minimize the secondary musculoskeletal complications of CMT [3]. Typical musculoskeletal complications of CMT in terms of craniofacial asymmetries include depression of the frontal bone and zygomatic arch on the CMT side, posteriorly positioned ear on the CMT side, deformational plagiocephaly on the non-CMT side, and deviation of the chin toward the non-CMT side [567].
The timing of surgery for CMT is an important factor that influences outcome. The best surgical outcomes are obtained before 5 years of age. In older individuals, surgical efficacy is reduced owing to irreversible musculoskeletal deformity. Most subjects with neglected CMT complain of secondary musculoskeletal deformities, in addition to pain and deficit of the neck motion for the remainder of their lives [8].
Although some studies suggest that surgical release of the SCM in neglected CMT is effective for cosmetic purposes, pain reduction, and functional improvement, there can be drawbacks. Based on our literature review, no report has been published on the natural history of craniofacial asymmetry of subjects with neglected CMT as they age. If the craniofacial asymmetry in subjects with neglected CMT worsens even after growth cessation, the progression of craniofacial asymmetry needs to be decelerated through surgical release, even for adults with neglected CMT.
The objective of this study was to evaluate the relationship between severity of craniofacial asymmetry and age in adults with neglected CMT by quantitatively assessing craniofacial asymmetry using craniofacial three-dimensional computed tomography (3D-CT).
MATERIALS AND METHODS
This was a retrospective study conducted in a single tertiary medical center. This research was approved by the Institutional Review Board of Ajou Medical Center.
Subjects
Among the subjects who visited the Clinic for Torticollis for the symptoms of abnormal head and neck postures between January 2009 and December 2013, subjects diagnosed with CMT who aged 18 years old or older at the time of craniofacial 3D-CT scan were included. Exclusion criteria were as follows: 1) subjects with a previous history of surgery or injection of botulinum toxin into the SCM for CMT; 2) subjects who had congenital disease that might incur craniofacial asymmetry, such as craniovertebral junction anomaly, segmentation anomaly of the vertebra, Goldenhar syndrome, Treacher Collins syndrome, and CHARGE syndrome, etc.
A diagnosis of CMT was made for the subjects who showed both of the following conditions: 1) shortening of the unilateral SCM, ending up with ipsilateral lateral flexion of the head and/or rotation of the chin toward the contralateral shoulder and 2) multiple or large low signal intensities within the SCM in magnetic resonance imaging, as previous described [9].
Craniofacial 3D-CT was performed when subjects showed grossly obvious craniofacial deformity due to neglected CMT. Craniofacial 3D-CT (scan parameters: 120 kVp, 400 mAs, scan time, 750 ms; matrix size, 512×512) was performed with multi-detector row helical CT (Philips, Eindhoven, The Netherlands). The CT scans were reviewed with a PiViewSTAR program (Infinitt, Seoul, Korea).
Limitation in range of neck motion and radiographic cervicomandibular angle were used for determining the clinical severity of CMT. A retrospective chart review of range of neck motion was performed for all cases. Range of neck motion was measured by using a handheld goniometer and was compared with that of the contralateral side to calculate the motion deficit. The cervicomandibular angle, defined as the angle between a line along the upper border of the C7 vertebral body and a line connecting the lower margins of the mandibular angle, was measured on the anteroposterior radiograph of the cervical spine to quantify the degree of head tilt [10].
Quantitative analysis of asymmetry on craniofacial 3D-CT
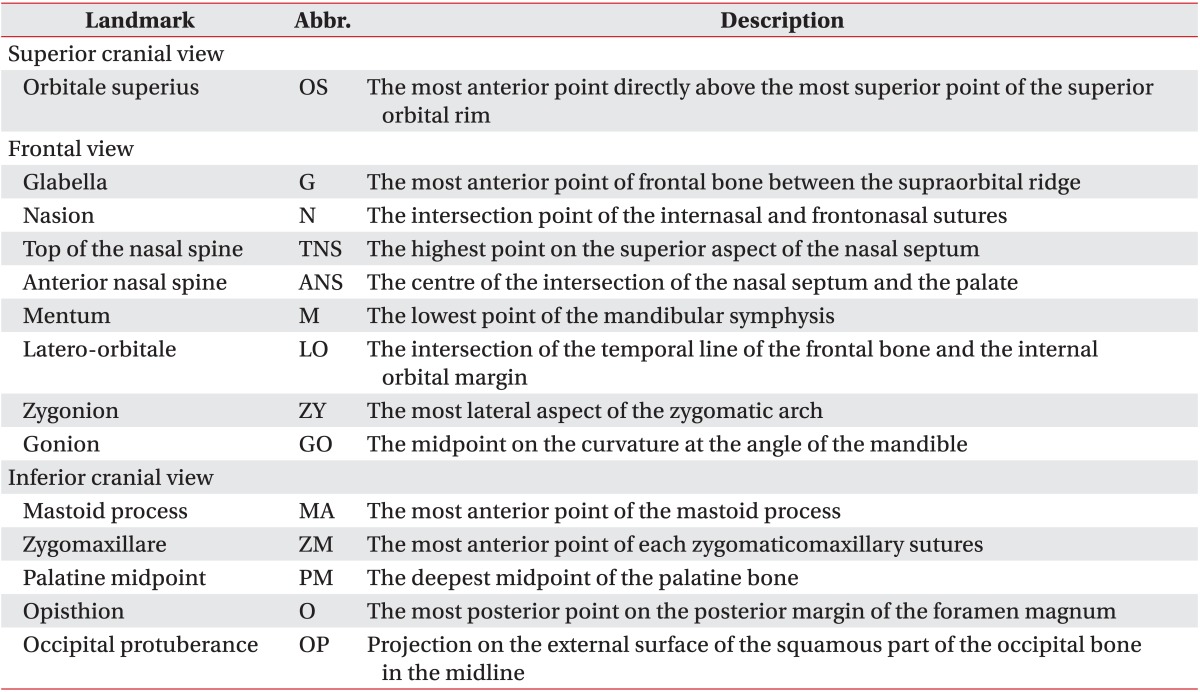
Anatomical landmarks were identified on one of three standard 3D-CT views (superior cranial, inferior cranial, and frontal views), which were vertical, caudal, and frontal surface projection images, respectively, based on the Frankfort horizontal plane [71112]. All the anatomical landmarks used in this study are described in Table 1. Quantitative measurements of asymmetry on craniofacial 3D-CT were independently and blindly performed by two of the first three authors. After inter-rater reliability was tested for quantitative measurement of craniofacial 3D-CT findings, the mean values measured by the two authors was used for linear regression analysis between craniofacial asymmetry and subject age.
Severity of cranial asymmetry
The cranial vault asymmetry index (CVAI) was used to measure the severity of plagiocephaly [1314]. The diagonal diameters were obtained from the orbitale superius (OS) directly above the most superior point of the superior orbital rim to the occipital landmark, which is defined by a parallel line directed posteriorly from the OS on the opposite side (Fig. 1A). CVAI (%) was calculated as [(longer diagonal shorter diagonal) / shorter cranial diagonal] × 100. Cranial asymmetry was considered significant if CVAI >3.5%, and was classified as mild (3.5%-7%), moderate (7%-12%), or severe (>12%).
Measurement of anteroposterior length asymmetry on the axial plane
Anteroposterior length asymmetry of the OS and zygomaxillare (ZM) was measured as shown in Fig. 1A and B. The frontal length ratio (FLR), b/a, represents the length asymmetry of the OS on the CMT side in comparison with that on the non-CMT side in the anteroposterior direction of the axial plane, in the superior cranial view. The z1-axis was defined as the coronal line perpendicular to the sagittal plane, which crosses the intersection of the 2 previously mentioned diagonals. The zygomatic length ratio (ZLR), d/c, represents the anteroposterior length asymmetry of the ZM on the CMT side in comparison with that on the non-CMT side, in the inferior cranial view. The z2-axis was defined as the line connecting the bilateral anterior margin of the mastoid processes (MA), and ZM is the most anterior point of each zygomaticomaxillary sutures.
Measurement of vertical length asymmetry on the coronal plane
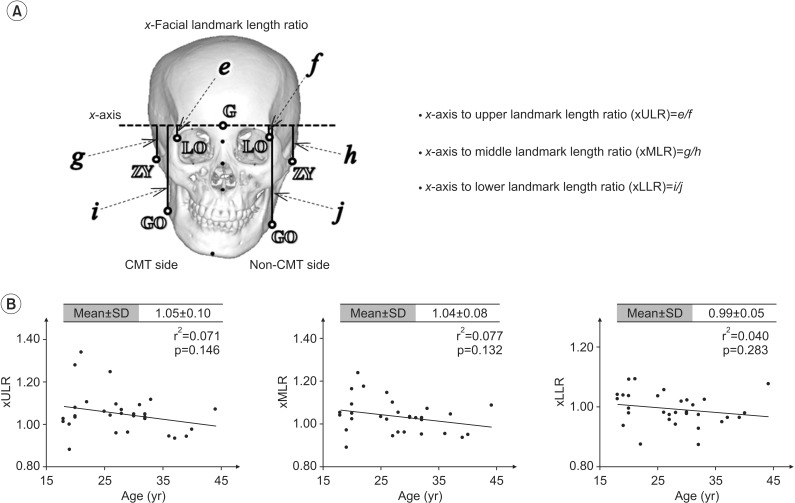
The vertical length asymmetry of the anterior facial landmarks was measured as shown in Fig. 2A. A mid-sagittal line was constructed by joining the landmarks, namely the glabella (G), nasion (N), and top of the nasal spine (TNS) to form the y1-axis, and the perpendicular line with origins at the G was defined as the x-axis in the frontal view. The x-upper landmark length ratio (xULR), e/f, represents the vertical length asymmetry of the latero-orbitale (LO), the intersection of the temporal line of the frontal bone and internal orbital margin from the x-axis on the CMT side in comparison with that on the non-CMT side. The x-middle landmark length ratio (xMLR), g/h, represents the vertical length asymmetry of the zygonion (ZY) on the CMT side in comparison with that on the non-CMT side. The x-lower landmark length ratio (xLLR), i/j, represents the vertical length asymmetry of the gonion (GO) on the CMT side in comparison with that on the non-CMT side. ZY is the most lateral point on the outline of each zygomatic arch, and GO is the mid-point on the curvature at the angle of the mandible.
Measurement of lateral length asymmetry on the coronal plane
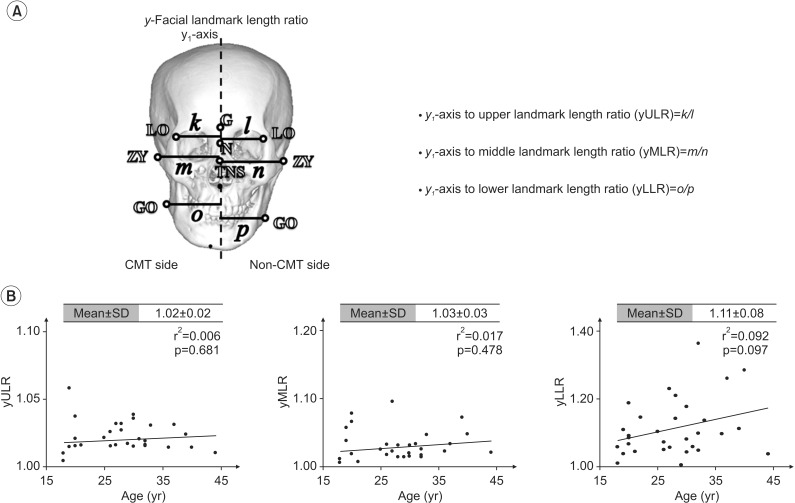
Lateral length asymmetry of facial landmarks LO, ZY, and GO was measured as depicted in Fig. 3A. The y-upper landmark length ratio (yULR), k/l, represents the lateral length asymmetry of the LO from the y1-axis on the CMT side in comparison with that on the non-CMT side. The y-middle landmark length ratio (yMLR), m/n, represents the lateral length asymmetry of the ZY on the CMT side in comparison with that on the non-CMT side. The y-lower landmark length ratio (yLLR), o/p, represents the lateral length asymmetry of the GO on the CMT side in comparison with that on the non-CMT side.
Measurement of vertical displacement on the coronal plane
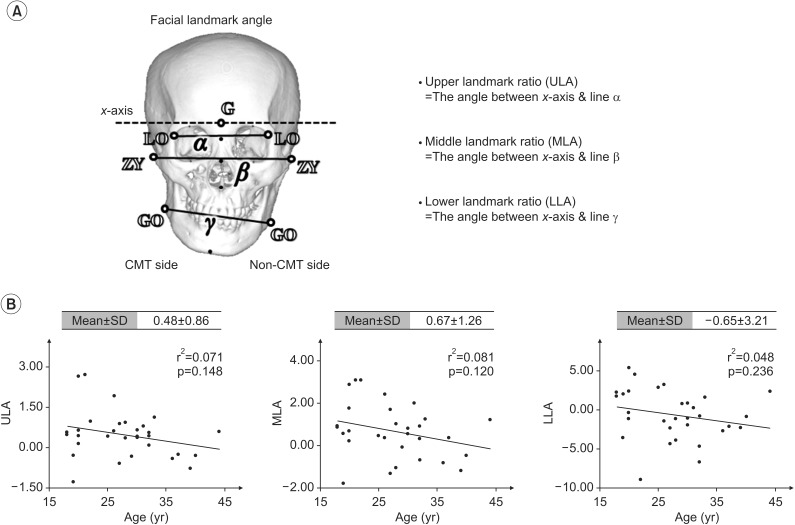
Vertical displacement of facial landmarks LO, ZY, and GO was measured as shown in Fig. 4A. The upper landmark angle (ULA), which represents the vertical displacement of the LO on the CMT side in comparison with that on the non-CMT side, is the angle between the x-axis and line α. The middle landmark angle (MLA), which represents the vertical displacement of the ZY on the CMT side in comparison with that on the non-CMT side, is the angle between the x-axis and line β. The lower landmark angle (ULA), which represents the vertical displacement of the GO on the CMT side in comparison with that on the non-CMT side, is the angle between the x-axis and line γ.
Measurement of mandibular rotation on the coronal and axial planes
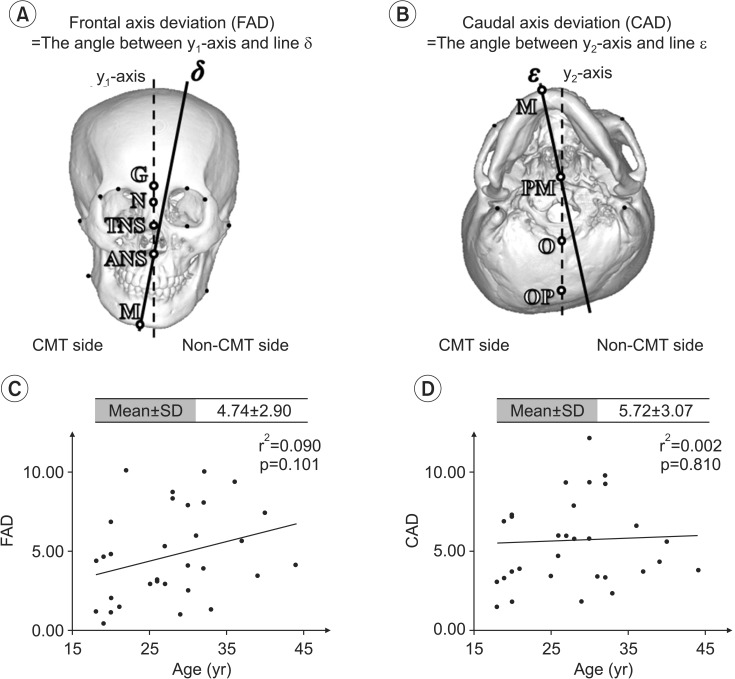
To measure the degree of mandibular rotation, the frontal axis deviation (FAD) and caudal axis deviation (CAD) were measured as shown in Fig. 5A and B. FAD is the angle formed by the intersection of the y1-axis and line δ, which represents the frontal mandibular axis defined by a line connecting the anterior nasal spine (ANS) and mentum (M) in the frontal view. CAD is the angle between the y2-axis and line ε, which represents the caudal mandibular axis. The y2-axis was defined by joining the landmarks occipital protuberance (OP), opisthion (O). The caudal mandibular axis was constructed by joining the landmarks M, and palatine midpoint (PM) in the inferior cranial view.
Statistical analysis
Statistical Package for the Social Sciences (SPSS) ver. 19.0 (IBM, Armonk, NY, USA) was used for the statistical analysis. The intra-class correlation coefficients (ICC) between the two investigators were calculated for inter-rater reliability. ICC scores >0.70 were considered reliable. Linear regression analysis was performed to evaluate the relationship between the cephalometric parameters and age of the subjects. If the relationship between cephalometric parameters and subjects' age was statistically significant in the simple linear regression analysis, a multiple regression analysis was performed, with covariates including limitation in range of neck motion or cervicomandibular angle. Statistical significance was set at p<0.05.
RESULTS
Characteristics of the subjects
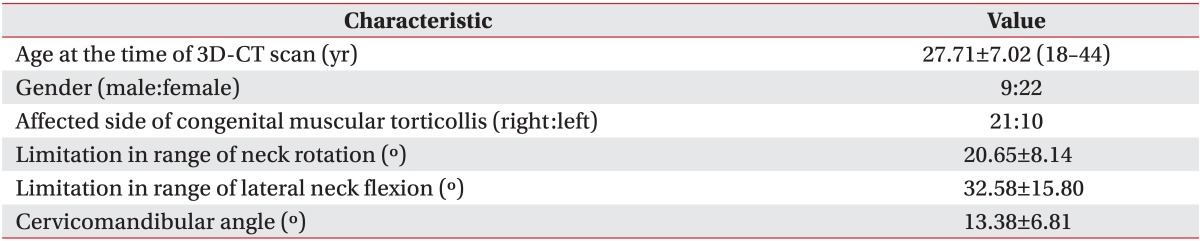
Thirty-one subjects (9 men and 22 women) who met the inclusion criteria were included in this retrospective study. The characteristics of the subjects are presented in Table 2. Age at the time of 3D-CT was 27.71±7.02 years (range, 18-44 years). The involved CMT side was the right in 21 subjects (67.7%) and left in 10 subjects (32.3%).
Quantitative analysis on craniofacial 3D-CT with inter-rater reliability
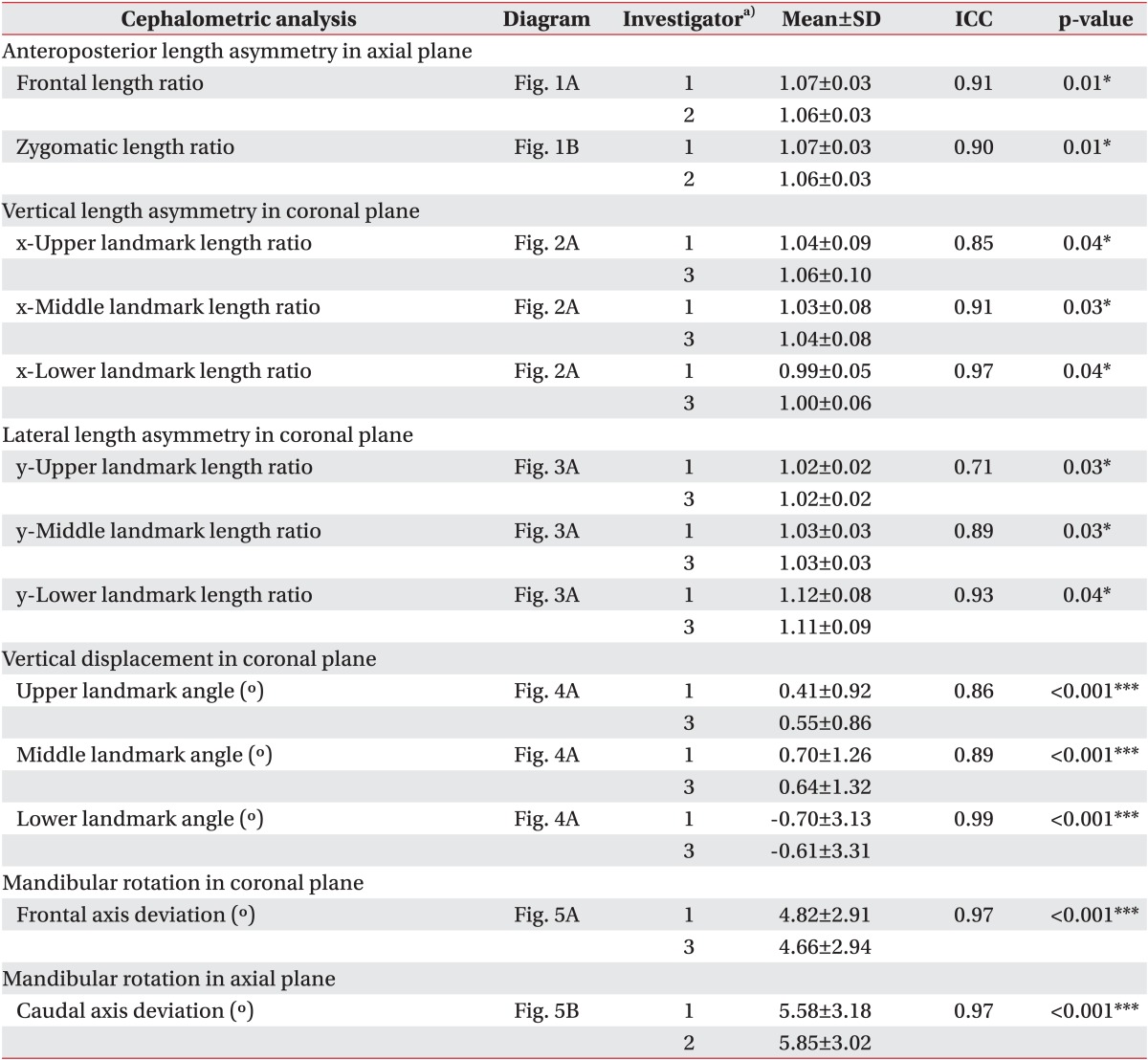
The results of the quantitative analysis of asymmetry on craniofacial 3D-CT as measured by the two investigators are presented in Table 3 along with the ICC values. All the ICC values were higher than 0.70, suggesting a good inter-rater reliability of all the measurements (p<0.05).
Severity of cranial asymmetry
Based on CVAI, 26 subjects (83.9%) had a significant cranial asymmetry, which include 8 mild cases, 17 moderate cases, and 1 severe case.
Anteroposterior length asymmetry on the axial plane
FLR (i.e., the anteroposterior length asymmetry of the frontal bone on the axial plane) was 1.06±0.03, which increased significantly with ages in the linear regression analysis (r2=0.176, p=0.019) (Fig. 1C). The relationship between the FLR and age was still statistically significant after adjusting for limitation in range of neck flexion and lateral flexion (adjusted r2=0.141, p=0.045) or cervicomandibular angle (adjusted r2=0.231, p=0.010). ZLR (i.e., the anteroposterior length asymmetry of the zygomatic arch on the axial plane) was 1.07±0.03, which also increased significantly along with age in the linear regression analysis (r2=0.188, p=0.015) (Fig. 1D). The relationship between the ZLR and age was still statistically significant after adjusting for limitation in range of neck flexion and lateral flexion (adjusted r2=0.227, p=0.019) or cervicomandibular angle (adjusted r2=0.426, p<0.001).
Vertical length asymmetry on the coronal plane
xULR, xMLR, and xLLR (i.e., the vertical length asymmetry of the anterior facial landmarks on the coronal plane was 1.04±0.09, 1.03±0.08, and 0.99±0.05, respectively. None of these was statistically significant with age in linear regression analysis (r2=0.071, 0.077, and 0.040, respectively; all p>0.05) (Fig. 2B).
Lateral length asymmetry on the coronal plane
yULR, yMLR, and yLLR (i.e., the lateral length asymmetry of the same paired landmarks on the coronal plane) was 1.02±0.02, 1.03±0.03, and 1.12±0.08, respectively. None of these was statistically significant with age in linear regression analysis (r2=0.006, 0.017, and 0.092, respectively; all p>0.05) (Fig. 3B).
Vertical displacement on the coronal plane
ULA, MLA, and LLA (i.e., the vertical displacement of the anterior facial landmarks on the coronal plane was 0.48±0.86, 0.67±1.26, and -0.65±3.21, respectively. None of these was statistically significant with age in linear regression analysis (r2=0.071, 0.081, and 0.048, respectively; all p>0.05) (Fig. 4B).
Mandibular rotation on the coronal and axial planes
FAD and CAD, which represent the deviation of the mandibular axis on the coronal and axial planes, were 4.82°±2.91° and 5.58°±3.18°, respectively. Both were not statistically significant with age in linear regression analysis (r2=0.090, p=0.101 and r2=0.002, p=0.810, respectively) (Fig. 5C and D).
DISCUSSION
To our knowledge, this study is the first to quantitatively evaluate craniofacial abnormalities, focusing on CMT patients aged 18 years or older. The aim was to evaluate the relationship between age and the severity of craniofacial asymmetry in patients with neglected CMT.
Craniofacial 3D-CT allows objective and quantitative assessments of the level of craniofacial asymmetry. Facial asymmetry is progressive if the contracted SCM is not released, although cranial asymmetry was already determined in patients younger than 6 months old [5]. However, the authors reported that the intercommissural angle was only measured by frontal photo analysis to represent facial asymmetry. Another study reported a correlation of the severity of craniofacial deformity with age, as analyzed using craniofacial 3D-CT images obtained from 14 CMT patients aged 1 month to 24 years [7]. However, most of the subjects were infants and juveniles, with only three adults.
The present study found a correlation of the severity of craniofacial asymmetry with age in terms of anteroposterior length asymmetry of the ipsilateral frontal bone and zygomatic arch on the axial plane in adult CMT patients. This may have reflected the ongoing shortening of the SCM on the affected side, which remains even after growth cessation. Unresolved traction force of the affected SCM and the contracted neighboring soft tissue may cause continuous mild torsion of craniofacial structures.
Inferiorly and laterally shifted facial landmarks on the CMT side on the coronal plane were noted (except vertical displacement of the GO), as well as a rotated mandibular axis toward the affected side on the coronal and axial planes. Unlike anteroposterior length asymmetry, none of these was considered progressive in the linear regression analysis with age.
We cannot fully explain this particular result on the axial plane, but it was observed that readings of the facial landmark length ratio and frontal mandibular axis deviation influenced the other readings. In case of, for example, right CMT, the GO level on the right side becomes raised with a considerable mandibular rotation toward the right side, which affects the estimation of the x-axis to the lower landmark length ratio (significant negative correlation was identified in the correlation analysis between the xLLR and FAD; r=-0.619 and p<0.001). In addition, there are possibilities of displacement underestimation of bilateral landmarks on the axial plane in the frontal view.
Although frontal photograph and simple radiographic analyses are performed to assess asymmetry in adult patients with CMT, in many cases they may not be enough to evaluate an anteroposterior length asymmetry, as shown in this study, which implies that 3D-CT may be beneficial.
There are pros and cons regarding treatments, surgical corrections inter alia, for adult patients who have neglected or unresolved CMT [15]. Many have refused such surgeries, taking into consideration the high rate of complications, marginal treatment effectiveness, and ongoing abnormalities. It is recognized that not all surgeries may result in the correction of craniofacial abnormalities, particularly for patients aged 5 years or older [161718]. Nonetheless, as recently reported, interest is increasing on those methods in view of the fact that any surgical correction may improve cosmetic and functional aspects along with the alleviation of pain related to it [8]. Others also reported improvement of cosmesis and range of neck movement after unipolar resection of the affected SCM [19].
According to the present study, surgical release of the affected SCM in neglected CMT patients may be required to prevent further exacerbation of craniofacial asymmetry, when the severity increases with age throughout the patient's adult life.
The strength of this study lies on the quantitative and objective analyses conducted based on 3D-CT data from the largest adult population with neglected CMT among studies regarding craniofacial asymmetry in CMT patients. The inter-rater reliability of the measurements between the two investigators was verified through an ICC test.
Limitation of this study is its retrospective nature, which may inherently contain the possibility of selection bias. Although this study had the largest targeted adult population among studies regarding craniofacial asymmetry in CMT patients, a longitudinal study targeting more subjects may lead to more precise results.
In conclusion, craniofacial asymmetry in terms of anteroposterior length asymmetry of the frontal bone and zygomatic arch on the axial plane became more severe with age even in the adults, based on the quantitative evaluation of 3D-CT images from 31 neglected CMT subjects aged 18 years or older. Assessment of anteroposterior length asymmetry on the axial plane seems to be the most accurate tool for measuring craniofacial asymmetry in adult CMT subjects. This finding may enhance our understanding of therapeutic strategies, such as careful monitoring and surgical release, to prevent progression of craniofacial asymmetry in adults with neglected CMT.

 XML Download
XML Download