

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Operative vaginal delivery is a labor management option that can avoid cesarean section in some specific situations, usually almost always at the end of the second stage [123]. When the scalp of the fetus is visible at the introitus or the leading point of the fetal head is placed over station +2 cm, operative delivery is performed if the delivery must be expedited due to the acute presentation of non-reassuring fetal heart rate monitoring or maternal exhaustion from prolonged labor [4]. In this advanced stage of labor, cesarean section carries an increased risk of maternal morbidity such as bladder injury or difficulty elevating the fetal head through the uterine incision because the fetus is far more advanced in the pelvic cavity [5]. Preparations for cesarean section including cooperation with anesthesiologists and other faculties are non-negligible and another reason to consider operative vaginal delivery.
Merriam et al. [2] reported that the rate of vacuum-assisted deliveries in the United States decreased slightly from about 6% in 2005 to 4% in 2013. In this population-based study, the factors related to the increased likelihood of operative delivery included diabetic disorders, nulliparity, labor induction, and chorioamnionitis. The well-known complications of operative deliveries are third- and fourth-degree birth canal lacerations and acute perinatal morbidities such as scalp lacerations, cephalohematoma, and subgaleal hemorrhage [467891011]. These adverse outcomes after operative delivery often become a troublesome for physicians despite successful vaginal delivery. Moreover, it is difficult to convince the patients and family members about the consequences despite the unclear association between neonatal complications and operative delivery. Thus, it would be helpful if the prediction of operative delivery before the initiation of labor is possible.
Numerous trial of labor studies have examined the success of vaginal delivery and the rate of cesarean sections [12]; however, attempts to predict operative delivery are lacking, and studies are usually limited to the identification of risk factors in a large population or meta-analysis [51314]. Several studies reported that an increased mid-trimester cervical length (CL) was associated with a higher risk of cesarean section [15161718]. Nevertheless, there are conflicting results of the association between a longer mid-trimester CL and the rate of cesarean delivery unlike the relationship between a short CL and the likelihood of preterm birth [192021].
The idea to investigate the association between mid-trimester CL and vaginal delivery failure during trial of labor started from the hypothesis that a cervix that does not shorten during the second trimester might be an obstacle or predisposition for an ineffective progression of labor. This study was designed to determine if the use of vacuum-assisted delivery and not only the likelihood of emergency cesarean section after trial of labor is associated with mid-trimester CL. Kahrs et al. [13] studied several sonographic findings to predict the success of vacuum-assisted deliveries; however, the ultrasonographic evaluations were performed only in nulliparous women who were diagnosed with a prolonged second stage of labor.
This study aimed to determine whether mid-trimester CL is associated with the rate of operative delivery.
Materials and methods
1. Study design
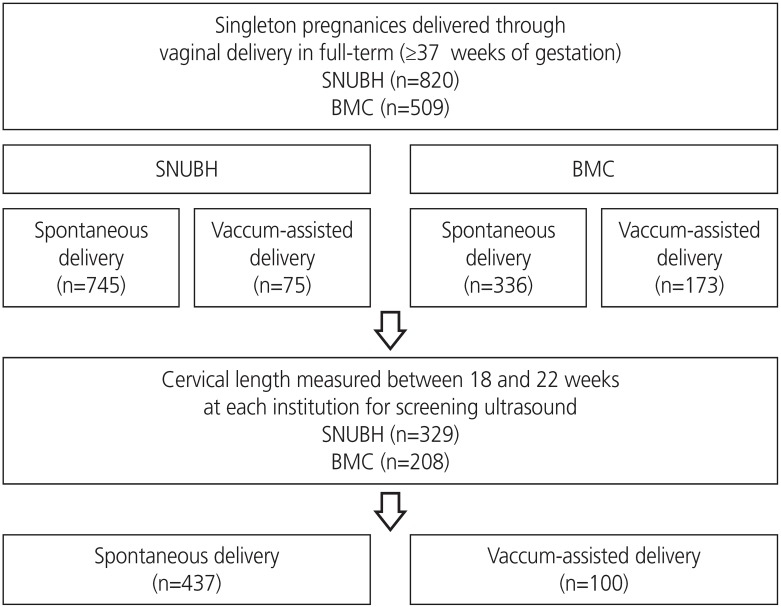
This retrospective study included consecutive women who achieved vaginal delivery at Seoul National University Bundang Hospital (SNUBH; n=820) or Boramae Medical Center (BMC; n=509) between January 2017 and February 2019. Only singleton pregnancies delivered at or beyond 37 weeks of gestation were included; multifetal pregnancies and cases of fetal death in utero were excluded. Among them, those for whom reliable data on CL measured at 18–22 weeks of gestation for the purpose of screening for the risk of preterm birth in each institution were analyzed (n=537) (Fig. 1). The study group was divided into 3 groups according to every 1 cm of CL.
2. Mode of delivery
Birth attendants at both institutions used vacuum assistance only; forceps were used in no cases. The vacuum cups used in the study population were soft or metal; however, the tool used in each case could not be identified through the medical records. Once the cup was placed atop the fetal scalp by the physician, the device created gradual vacuum pressure until the total negative pressure reached 300 mmHg.
3. Significant variables to determine risk factors
Obstetric and medical factors with a possible association with operative delivery were identified and analyzed. Information was collected on maternal characteristics including age, parity, mid-trimester CL, gestational age at the time of CL measurement, hypertensive disorder, diabetic disorder, body weight, and height at delivery. Obstetric conditions such as the use of intravenous oxytocin for labor induction or augmentation of spontaneous labor pain, the application of epidural anesthesia, gestational age at delivery, and neonatal birthweight were reviewed in the medical records.
4. Statistical analysis
Data were tested for normality using the Kolmogorov-Smirnov test. Continuous variables were compared using the Mann-Whitney U test or Kruskal-Wallis analysis. The proportions were compared using Fisher's exact test or the χ2 test. Logistic regression was used to determine the association between mid-trimester CL and vacuum delivery. Multivariate analysis was then performed to adjust for variables confounding the outcomes and identify risk factors. P-values <0.05 were considered statistically significant, and the analysis was performed using SPSS version 22 (IBM SPSS Inc., Armonk, NY, USA).
Results
Fig. 1 shows the study population from each institution. Only term pregnancies were included because vacuum delivery is less often recommended in preterm births due to the high incidence of hemorrhagic complications such as intraventricular hemorrhage. Among the 1,329 singleton pregnancies (820 in SNUBH and 509 in BMC), data for the mid-trimester CL measured during a routine ultrasound examination were available for 537 pregnancies. Among them, 18.9% (100/537) of the patients underwent vacuum-assisted vaginal delivery.
Various factors were compared according to the use of vacuum assistance (Table 1). The proportion of nulliparous women was significantly higher in the vacuum-assisted delivery group than in the spontaneous delivery group (79.0% vs. 49.4%, P<0.001). The median CL and gestational age at the time of the measurement were comparable. The proportions of cases in which intravenous oxytocin was used for induction or to augment labor or uterine contractions and the application of epidural anesthesia were both significantly higher in the vacuum-assisted delivery group than in the other group (both P<0.001). The mean neonatal birthweight did not differ between groups.
Table 1
Clinical characteristics and pregnancy outcomes of the study population according to the mode of delivery
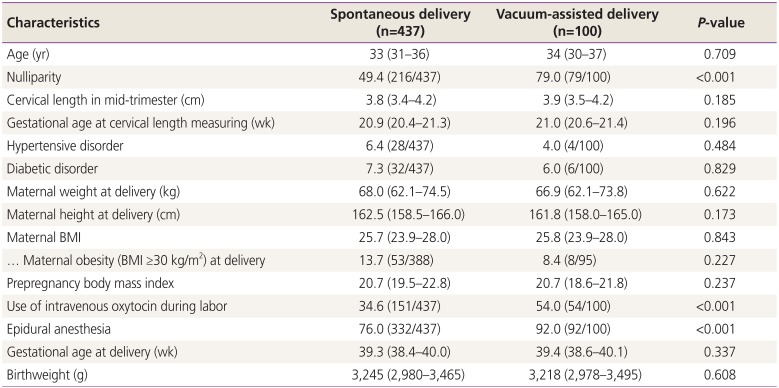
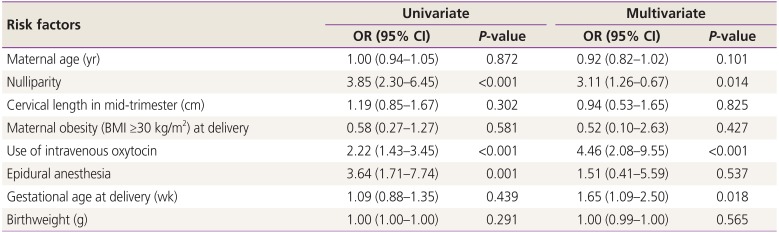
Table 2 shows the risk factors and associations with vacuum use analyzed by logistic regression analysis. In the univariate analysis, nulliparity, intravenous oxytocin use, and epidural anesthesia use were associated with vacuum-assisted delivery. However, in multivariate analysis, epidural anesthesia was not associated with vacuum use; otherwise, nulliparity and intravenous oxytocin use remained significant risk factors after the adjustment for other factors. Moreover, gestational age at delivery was associated with vacuum-assisted delivery in multivariate analysis. Mid-trimester CL was not associated with vacuum use in the logistic regression analysis.
Table 2
Risk factors of vacuum-assisted delivery analyzed by logistic regression analysis
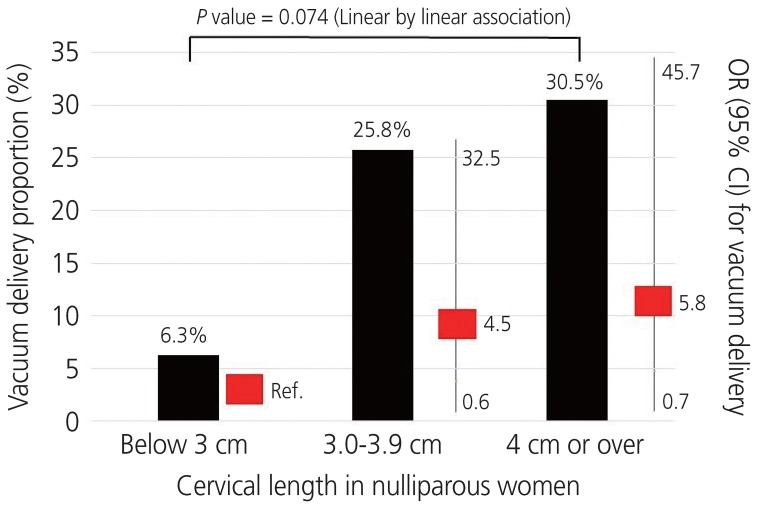
In only nulliparous women, the rates of vacuum use were compared by every 1 cm of CL for easier application in clinical settings (<3 cm, 3.0–3.9 cm, and ≥4 cm). In the groups with a CL of 3.0–3.9 cm and ≥4 cm, the rates of vacuum-assisted delivery were 25.8% (41/159) and 30.5% (36/118), respectively, higher than that of the group with a CL of <3 cm (6.3% [1/16]) (Fig. 2). The P-value on the analysis of a linear by linear association was 0.074, while the P-values of the differences among groups in the post hoc analysis were all below 0.05. The odds ratio (OR) was 4.5 (95% confidence interval [CI], 0.6–35.2; P=0.156) and 5.8 (95% CI, 0.7–45.7; P=0.098) using the group with a CL of <3 cm as the reference value for the logistic regression analysis. Both were higher than that of the group with a CL <3 cm; however, the difference was not statistically significant.
Discussion
The principal study findings were as follows: 1) Mid-trimester CL was not associated with vacuum assistance during delivery; 2) Nulliparity, gestational age at delivery, and intravenous oxytocin use were independent risk factors for vacuum delivery in full-term singleton pregnancies on multivariate regression analysis; 3) When the population was divided into 3 groups by every 1 cm of CL, the proportion of vacuum deliveries increased as the measurement increased; however, the difference did not reach the statistical significance.
A short mid-trimester CL is a well-known independent risk factor for preterm birth; therefore, the universal screening of mid-trimester CL is recommended to identify cases at high risk of preterm delivery [192122232425262728]. Similar to the association between cervical shortening and early spontaneous delivery, researchers consequently hypothesized that a longer CL would be associated with prolonged pregnancy (post-term delivery) or difficult spontaneous delivery [293031]. A few studies have examined the relationship between CL at term or immediately before delivery and vaginal delivery success [532]. Ramanathan et al. [32] demonstrated that, when the CL was ≥4 cm at 37 weeks of gestation, 89% (8/9) of nulliparous women underwent cesarean section after trial of labor due to failure to progress or fetal distress. One meta-analysis demonstrated that CL before labor induction did not predict the mode of delivery or induction success [12].
Smith et al. [18] demonstrated a relationship between cesarean section rate and the CL measured at 23 weeks of gestation. They divided the subjects into quartiles by mid-trimester CL; the reported OR for cesarean section in the fourth quartile was 1.81 (95% CI, 1.66–1.97) compared to the first quartile. Miller et al. [15] reported the increased mid-trimester CL was significantly associated with a higher frequency of cesarean section in singleton nulliparous women. In the study, the frequency of cesarean section increased with odds of 20.3% for every additional centimeter of CL. Van de Mheen et al. [17] performed a similar study on twin pregnancy; however, the mid-trimester CL was not associated with a risk of cesarean section. Unlike that study, Sung et al. [16] reported that a longer CL in mid-pregnancy was a risk factor for cesarean section in twins and higher rates of cesarean deliveries as the quartiles of the study population increased.
Although the related relationships between sonographically measured CL values and trial of labor success are conflicting, many researchers have explored the possibility of applying CL to other additional obstetric outcomes rather than to predict preterm birth. As a diagnostic tool, measuring CL is a non-invasive, relatively easy, and widely used technique. Operative deliveries such as those using vacuum assistance avoid cesarean section; however, because of the increased rates for higher-degree lacerations of the birth canal and several neonatal complications such as cephalohematoma and subgaleal hematoma, birth attendants might prefer cesarean section in the clinical setting to reduce the chance of post-procedural risks. From this point of view, an effective tool to predict difficult deliveries or need for vacuum assistance must be identified.
The main strength of this study is that it attempted to discern the association between mid-trimester CL and vacuum-assisted delivery. The study population was drawn from 2 different institutions, and the sample size was adequate because pure were used of relatively low-risk singleton pregnancies. However, it is limited by its retrospective nature. Future prospective studies on the rates of operative deliveries for various conditions of the population are required to identify a model for predicting difficult vaginal deliveries.
In conclusion, mid-trimester CL is not a useful predictor for future vacuum-assisted delivery in cases of successful term vaginal deliveries.
 XML Download
XML Download