

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Puerperal genital hematomas, rare complications of childbirth, are obstetric ailments with an incidence of 1/500 to 1/12,500 that can occur spontaneously or as a result of episiotomy. Most cases are associated with operative delivery. Of all genital hematomas, 1/1,000 require surgical intervention. Such hematomas usually form as a result of damage to the anterior iliac artery, which usually has a vaginally rich anastomotic network [1]. The risk factors for puerperal genital hematomas include delivering a large baby, perineal tearing, nulliparity, rapid delivery, and use of instruments at birth [2]. Cases of intrapartum vulvovaginal hematoma can involve excessive blood loss. If a puerperal hematoma develops, the bleeding may be fatal if the patient is not hemodynamically stable. There are many methods for treating puerperal hematomas; they include observation, surgical drainage, bleeding vein ligation, and vaginal compression with gauze tamponade. Rectal buffer, hysterectomy, and internal iliac artery ligation are less popular treatment methods. Angiographic embolization is a newer technique. Here, we present a case wherein we treated a common hematoma that formed in a mediolateral episiotomy line using the vacuum-assisted closure (VAC) technique. We used the VAC system in this case because normal wound healing could not occur and secondary suturing failed.
Case report
A 23-year-old 39-week pregnant woman (gravida 1, parity 0) presented to the health center in labor. In the first examination, the cervical dilatation was 5 cm, effacement was 80%, and station was 0. The patient was taken to the delivery room. Approximately 5 hours after the onset of labor pains, she gave birth to a live baby weighing 3,560 g and 48 cm long with the aid of a mediolateral episiotomy. After episiotomy repair, the patient was followed up but required re-evaluation in the operating room under anesthesia due to increased vaginal bleeding and tachycardia. A 7-cm hematoma pressing upon the rectum was detected in the episiotomy line, which was opened for suturing of the bleeding vessels. The patient was given 5 units of red blood cells and 3 units of fresh frozen plasma. However, during follow-up, she was admitted to our referral clinic with increasing hematoma size and impaired hemodynamics. Blood tests revealed the following: hemoglobin, 7.4 g/dL; platelets, 38,000/mm3; and fibrinogen, 100 mg/dL. Vital parameters included: pulse, 140/min; blood pressure, systolic 80 mmHg and diastolic 40 mmHg; fever, 35.5°C; and oxygen saturation, 85%. Her estimated blood loss was 3,000 mL.
The patient was diagnosed with a rectovaginal hematoma and treated surgically. The sutures in the episiotomy line were about to rupture (Fig. 1A). Thus, the hematoma in the vagina (depth, approximately 20 cm) was explored and evacuated and the bleeding veins were sutured. The bleeding was controlled and the incision line was closed. During these procedures, the patient was given 9 units of red blood cells, 7 units of fresh frozen plasma, and 2 units of fibrinogen concentrate. On the 7th postoperative day, the patient's sutures opened, the wound was debrided, the wound site was cultured, and appropriate antibiotic therapy (ceftriaxone, metronidazole) was started according to the culture results (Fig. 1B). The wound was debrided and irrigated twice daily and wound care continued until the 10th day postpartum.
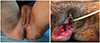
Fig. 1
(A) Episiotomy sutures about to rupture prior to hematoma drainage. (B) Wound dehiscence of episiotomy before vacuum-assisted closure.
We decided to apply an alternative treatment model, VAC, because the healing process was very slow and the affected tissue was deep. At the beginning of the VAC application, a Foley catheter was placed in the urethra. Green sterile sponges composed of polyurethane and polyvinyl alcohol cut according to the defect size were counted and placed into the defect. A waterproof adhesive material was placed around the anus to create a dry, flat area. Adhesive tape was applied to close the vaginal opening between the mons pubis and inner legs, while the anal channel was left open (Fig. 2A and B). The adhesive tape was cut from the anus to facilitate the passage of feces, and the VAC was operated at 125 mmHg. Air leaks were re-taped. No fecal or urinary contamination occurred. The VAC was changed every 3 days until the 10th day. During each VAC replacement, the wound was debrided and irrigated. Antibiotic therapy and a prophylactic dose of enoxaparin were adm inistered. Mobilizing the patient with VAC was problematic; she was able to walk comfortably. The patient expressed intense pain during the VAC exchange and underwent the procedure under mask anesthesia. On the 10th day of VAC treatment, the defect was completely closed and the perineum had an opening of about 3 mm (Fig. 2C). No fecal or urinary incontinence was observed. The patient was discharged on the 21st postoperative day.

Discussion
Defects in the episiotomy line are a serious medical problem that can cause physical and psychological problems. Different treatment modalities have been applied for this purpose. The VAC model, first described in 1993 and developed by Argenta and Morkywas in 1997, accelerates wound healing by creating negative pressure [34]. Although its mechanism is unclear, the widely accepted view is that it promotes angiogenesis, reduces local edema, increases cellular mitosis, and reduces inflammation. Its mechanical action enhances granulation and proliferation [56].
VAC therapy is commonly used to treat open abdominal wounds, diabetic ulcers, chest injuries, and orthopedic surgery sites. It has also been used to treat soft tissue infections and defects after compartment syndrome in burn patients. However, data provided to date on its use to treat perineal injuries have been provided in case reports only. With VAC treatment, the rapid progression of granulation tissue in open perineal wounds, shrinkage in irregular wound area, and significant reduction in hospital stay have been reported [7]. Narducci et al. [8] reported that the use of VAC application for 11 days immediately after vulvectomy reduced the total duration of the cicatrization by about 16 days. Similarly, Aviki et al. [9] reported that applying VAC to perineal damage after vaginal delivery using forceps both accelerates tissue healing and shortens hospitalization time.
Vaginal and perineal injuries are normally surrounded by damp tissue and have irregular edges that limit wound healing. Due to the close proximity of the anus and the urethra, chronic exposure of these wounds to fecal and urinary matter contaminates wounds and prevents healing. Despite the anal incontinence in our case, the waterproof adhesive tape we placed around the anus protected the wound site against contamination. In this case study, we showed the effect of VAC use on the healing of a 20-cm-wide perineal wound whose risk of contamination was higher than that of other regions.
For wounds and wound infections that do not heal normally, VAC use can accelerate and control healing by providing continuous negative suction pressure as a noninvasive active treatment. VAC treatment is widely used by surgeons after plastic and reconstructive surgeries.
In conclusion, our findings demonstrated that VAC therapy is a reliable method for draining infections, increasing granulation tissues, and reconstructing large perineal defects. However, a future series with a greater number of patients is needed to better evaluate treatment outcomes.
 XML Download
XML Download