

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Allergy to peanuts and tree nuts (TN) are often severe, may be life threatening and even fatal [123]. The prevalence of these allergies is increasing [4] placing an increasing burden on children and families. There is also a significant impact on quality of life for children with nut allergies [5]. Presently the standard of care for children with peanut or TN allergy is avoidance of the food [6]. Therefore predicting whether an individual child's allergy remains persistent over time is important but equally important is identifying those children whose allergies resolve over time.
Studies have shown that individuals with peanut allergy who report severe initial reactions are more likely to report severe subsequent reactions [7]. For peanut the size of the skin prick test at the time of ingestion may have some predictive value in terms of predicting the risk of anaphylaxis [8]. In retrospective, questionnaire based, studies some nut allergic patients reporting mild or moderate reactions do report subsequent severe or even life-threatening reactions [9]. For this reason it is generally accepted that all nut allergic individuals should be prescribed an adrenaline autoinjector even if there is no history of anaphylaxis. However, many patients do not carry their adrenaline autoinjectors or use them appropriately [10].
A number of previous studies have examined the relationship in terms of severity between initial and subsequent allergic reactions to peanut. However, in these studies the severity of either the initial or subsequent reaction or both was determined by history and patient report rather than prospectively by controlled oral food challenges (OFCs) [27111213141516]. In addition there are limited studies examining the progression of TN allergy [17].
A particularly difficult group to manage from the available data are those peanut or TN allergic children with a history of only mild reactions or higher threshold doses. The aim of this cohort study was to prospectively describe changes in reaction severity and threshold dose on repeated OFC in peanut and TN allergic children and to identify any factors that may predict improvement or worsening of clinical allergy over time.
MATERIALS AND METHODS
The allergy service at Sydney Children's Hospital maintains a database from children attending the allergy clinics and those undergoing OFCs. This database was queried to produce a list of patients that had previously undergone OFCs for peanut or TN. Ethics approval was obtained through the South Eastern Sydney Illawarra Area Health Service Northern Hospital Network Human Research Ethics Committee (ref No. 08/010) prior to any contact with families.
Study cohort
This study was conducted between February 2011 and December 2012. The selection criteria included children who had been referred from the Sydney Children's Hospital Allergy Clinic for a peanut or TN OFC between January 2006 and December 2011. To be eligible, children must have developed a nonanaphylactic reaction after ingesting a cumulative dose of at least 4 g of whole nut (peanut or relevant TN) during the OFC. The first OFC must have occurred 12 months or more before the proposed date of the 2nd (study) OFC. Eligible children were sent an expression of interest form inviting them for a second OFC with the same food. Research information was discussed with families who returned this form and agreed to participate. Written informed consent was obtained from parents or guardians when families presented for their second OFC. Those children, who had either reacted to a cumulative dose lower than 4 g, showed tolerance or who developed anaphylaxis during the first OFC were excluded. No children were excluded based only on the size of their SPT at either the initial or study OFC and serum specific-IgE levels were not routinely measured. Eligible families who did not respond to the initial letter within four weeks were contacted by telephone.
Oral challenges
Referral for the initial OFC was at the discretion of the treating clinician based on the patients' clinical history and skin test results. Until 2010, the protocol used for the OFC involved the children ingesting cumulative doses of peanut or TN, usually starting at 0.2 g of whole nut and ending with a maximum possible cumulative dose of 12.2 g of whole nut. After 2010 the protocol was changed to start at 0.6 g and to build up to a maximum possible cumulative dose of 19.35 g. Thus the minimum cumulative threshold dose consumed by any subject during the first OFC was 4 g and the maximum was 19.35 g (mean, 9.94 g). The second OFC (study OFC) was performed at least 12 months after the 1st using the post 2010 protocol. Subjects were asked to consume an amount at least equal to that which had triggered the reaction during their first OFC (unless a reaction occurred earlier that required that the challenge be terminated), and those that had not developed a reaction despite consuming that amount were given the option of continuing. Thus some subjects consumed more of the challenge food during the study OFC than they had during the first OFC. If they completed the study OFC without a reaction their allergy was deemed to have resolved.
Definitions and stopping criteria
We used the Australasian Society of Clinical Immunology and Allergy definition of anaphylaxis [18]. Asthma and eczema were defined as parent-report of a doctor-diagnosis. Participants were considered allergic to aeroallergens if they had a positive SPT and an associated clinical condition e.g., asthma or allergic rhinitis. Allergy to other food or nut was defined as a positive SPT with or without a past history of reaction. Stopping criteria for OFCs were based on objective clinical symptoms such as urticaria (not limited to the perioral region), angioedema, vomiting, cough, wheeze, etc. OFCs were also stopped if severe subjective symptoms occurred such as severe abdominal pain or nausea and the participant or their parent(s) refused to continue.
Groups
Participants were divided into groups by comparing the outcome of the peanut or TN OFC performed for the study (2nd OFC) with the outcome of the preceding OFC performed during the initial workup of the patient's allergy (1st OFC). If during the 2nd OFC any of the following criteria were met the patient was classified as 'better': (1) the clinical severity grading of a reaction (according to Sampson [19]) was lower than during the 1st OFC; (2) the threshold (i.e., cumulative dose of nut) that elicited the reaction increased; or (3) both remained unchanged. Conversely if the clinical severity grading (1) worsened, (2) the threshold decreased or (3) both, the patients' were classified as 'worse'. Then the 'better' patients who completed the 2nd OFC and did not react at all were regrouped as 'resolved' for comparison with those whose allergy was 'persistent'. The 'persistent' group therefore consisted of 3 patients from the 'better' group who all developed less severe reactions but still reacted and the 13 children from the 'worse' group (Fig. 1).
Statistical methods
Categorical data between groups were compared using the chi-square test while continuous data were compared using either the Student t-test for parametric or the Mann-Whitney U test for nonparametric data. Where relevant, paired variables for the 1st and 2nd OFC were compared within groups using paired t-tests or Wilcoxon signed rank test. Receiver operating curve (ROC) analysis was used to determine cut-offs of the SPT for predicting the outcome of the 2nd OFC. This analysis was performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). A p-value of <0.05 was considered statistically significant.
RESULTS
Patient characteristics
Overall 87 families were invited to participate. Twenty-six were finally recruited for the study (response rate of 29.9%). Common reasons for nonparticipation included that the child was now reportedly tolerating the food and/or that the child refused to undergo another OFC. There were no demographic differences between those who participated and those who declined (data not shown). Both the severity of reactions and/or the threshold dose varied substantially between the first and second OFC for the majority of participants. Peanut or TN allergy had persisted in 16/26 (61.5%) and resolved in 10/26 (38.5%) of participants (Fig. 1). Furthermore only 3/16 (18.8%) of those who persisted had 'improved' (higher threshold dose in one subject) or remained stable (threshold dose and severity of reaction unchanged from the 1st to the 2nd OFC in two subjects). The remaining 13/16 (81%) 'worsened' between the 2 challenges with 10/13 reacting to a lower threshold dose and 3/13 both reacting to a lower threshold dose and having more severe reactions. Two of these subjects developed anaphylaxis during their 2nd challenge. The median age of the first clinical reaction (not the first in-hospital OFC) for all participants was 27 months (range, 7-132 months). Mean age at the first in-hospital OFC was 5.9 ± 2.5 years and at the second was 8.9 ± 2.7 years. The mean time interval between the first and the second OFC for all participants was 35.5 ± 16.5 months (range, 12-72 months). Between the 1st and 2nd OFC 25/26 subjects (96%) had been avoiding the relevant nut but had been consuming foods labelled "may contain traces of nuts". Challenges were conducted with peanut in 17 cases (65.4%) and TN in 9 (34.6%; Walnut 5, Hazelnut 2, Cashew 2). The final grouping of the subjects is shown in Fig. 1.
Factors predicting outcome
Grouping as 'better' or 'worse'
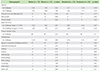
When the participants were grouped as better or worse, there was a significant difference only in the age at which the child had their first clinical reaction to the particular nut (p = 0.02) (Table 1). The median age at first clinical reaction for those that worsened was lower compared with those that improved. More children in the 'worse' group were allergic to nuts other than the nut to which they were challenged but this difference did not quite reach significance (p = 0.063) (Table 1). There were no other demographic features or co morbidities that were predictive of outcome for this grouping. We tried to describe a cutoff of the SPT wheal size prior to the initial OFC that could predict the outcome of the second OFC for this group. ROC analysis revealed that the SPT was a poor test overall with an area under the curve (AUC) of 0.52. A mean SPT wheal size for the relevant nut prior to the initial OFC of 6 mm had 92% sensitivity and 77% specificity for predicting the outcome of the 2nd.
Grouping as 'resolved' or 'persistent'
Once again those whose allergy persisted were significantly younger when they had their first reaction (Table 1). Similarly children whose allergy persisted reacted more quickly during the 1st OFC but the difference was not statistically significant (Table 1). ROC analysis for this grouping revealed that the SPT was once again a poor test with an AUC of 0.55. A mean SPT wheal size for the relevant nut prior to the initial challenge of 6 mm had 94% sensitivity and 70% specificity for predicting the outcome of the 2nd challenge.
Paired results
Table 2 shows the results when paired variables were analysed firstly for those subjects in whom the allergy persisted (n = 16) or worsened (n = 13), and secondly those in whom the allergy resolved (n = 10), comparing the 1st to the 2nd OFC. Interestingly there was no increase in the mean SPT wheal size prior to the 2nd OFC compared with prior to the 1st in those that persisted and/or worsened; and in fact there was even a nonsignificant decrease. However, there was a significant decrease in the mean SPT wheal size prior to the 2nd OFC compared with the 1st if the allergy 'improved' or resolved. Similarly there was a significant decrease in both the median threshold dose and the time to the reaction during the 2nd OFC compared with the 1st in those subjects in whom the allergy persisted and/or worsened. These two variables could not be compared if the allergy resolved because no reaction occurred in this group during the second OFC.
DISCUSSION
This paper describes repeated PN and TN OFC outcomes in a cohort of children unselected on the basis of SPT size and with initial 'mild/moderate' reactions and high threshold doses. A number of previous studies describe the severity of initial and subsequent reactions to peanut and in some cases TN but either did not use controlled OFCs at both time points or participants were selected based on SPT or specific-IgE results [711121314151617]. In addition the current study included both peanut and TN allergic children and there are few studies describing the progression of TN allergy [17].
We selected children based only on their nonanaphylactic clinical history and did not exclude any for OFC regardless of their pre-OFC SPT results and found a resolution rate for PN and TN allergy of 38.5%. Skolnick et al. [14] reported resolution of peanut allergy in around 20% of a cohort of children selected for peanut specific-IgE levels < 20 kU/L. And subsequently Fleischer et al. [11] demonstrated that up to 55% of children selected on the basis of peanut specific-IgE levels < 5 kU/L developed tolerance. Thus it may be necessary to repeat OFCs in selected nut allergic children to demonstrate that tolerance has developed. Especially as it has been reported that recurrence rates of peanut allergy are higher if peanut is avoided once tolerance has been achieved [20].
Fleischer et al. [11] found a significant difference in peanut specific-IgE levels at repeat OFC between children who became tolerant and those that did not. Further studies have defined cutoffs of SPTs and specific-IgE levels that are predictive of clinical nut allergy at the time of OFC [212223]. However, they have not examined whether initial tests can be used to predict changes over time. In the current study there were no differences in mean SPT size between groups at the time of challenge. However, individually those whose allergy improved showed a significant drop in SPT wheal size between the first and second OFC. In this cohort a mean SPT of 6 mm at the first OFC was found to have good sensitivity for predicting improvement by the second.
Interestingly most children in this study whose nut allergies persisted actually 'worsened' during their 2nd challenge compared with the first (81%) and two children in this group developed anaphylaxis on rechallenge. In addition it was found when allergy persisted the subsequent reaction was significantly more likely to occur at a lower threshold dose and more rapidly than the first.
Current asthma, adolescence, low threshold dose and the size of the SPT have been associated with an increased risk of anaphylaxis and even fatal reactions [1234823]. In the current study these variables were not associated with the likelihood that nut allergy in an individual child would resolve or worsen. However, we did show data to suggest that children who are younger at the time of their first allergic reaction may be at increased risk of persistent or worsening nut allergy over time.
There were a few potential weaknesses of this study. The response rate was low at ~30% and therefore may have been subject to selection bias. The study called for children who had reacted to peanut or TN during an OFC to return for a 2nd OFC. Many were reluctant to risk experiencing an unpleasant clinical reaction that was unlikely to change overall management. As a result recruitment was difficult and therefore the study was perhaps underpowered to detect significant differences between these groups. Secondly many of the children included in the 'worse' grouping had a decrease in their threshold dose for reactions rather than an actual worsening of symptoms. However, in a previous study we showed that peanut allergic children who continue to consume peanut beyond their initial reaction thresholds will in almost all cases develop anaphylaxis suggesting that a drop in the reaction threshold would be clinically relevant [8].
In conclusion, mild/moderate peanut or TN allergy resolved in over 38% of cases in this study. Conversely in those with persistent allergy there may be a significant risk of worsening of the clinical severity and/or a reduction in the threshold dose over time. Children who are younger when they experience their first reaction may be at increased risk. We were not able to identify any demographic features that were predictive of a change in the severity of allergic reactions over time. While this study included only a relatively small number of children and therefore larger studies may be needed, our findings suggest that children with a previous mild/moderate reaction should be regularly reviewed and offered repeat OFC when appropriate in order to guide clinical management.


 XML Download
XML Download