

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Caries, a common dental disease, is more prevalent in adolescents than in adults [1]. All patients should be screened for caries before and throughout orthodontic treatment. If a lesion is detected, it should be permanently restored and any pulpal involvement addressed before initiating treatment [1]. Therefore, prior to commencement of orthodontic treatment, it is necessary to treat all existing tooth caries. Caries can occur in pits and fissures and account for more than 60% of all lesions [23].
Operative dentistry has seen much progress in recent years in posterior teeth restoration, including a gradual movement towards resin composites, rather than dental amalgam, which has allowed the adoption of minimal intervention approaches that conserve and preserve remaining tooth tissues and structures [4]. There are no reasons why posterior composite restorations should not have long survival rates as long as patient, operator, and materials factors are all considered at the time of restoration. Many of the improvements achieved in today's materials have been realized through continuously reducing the size of filler particles incorporated in the resin matrix of commercial dental composites to the present nano-composite materials [56].
Nanofill resin composite that contains nanosized fillers and/or nanofiller clusters has been developed [7], while the microhybrid composites are based on the particles averaging about 0.4–1.0 μm in size. These materials are recommended for both anterior and posterior restorations based on their combination of strength and polishability [78].
To the best to our knowledge there are no data available on the clinical performance of occlusal carious restorations completed prior to the initiation of orthodontic treatment. Therefore, the aim of study was to evaluate the clinical performance of restorations for occlusal caries over 5 years, which were performed using nanofill and microhybrid composites in combination with 3-step etch-and-rinse adhesive and completed before orthodontic treatment. The null hypothesis tested was that there was no difference in the clinical performance between the 2 composites after 5 years.
MATERIALS AND METHODS
Study design
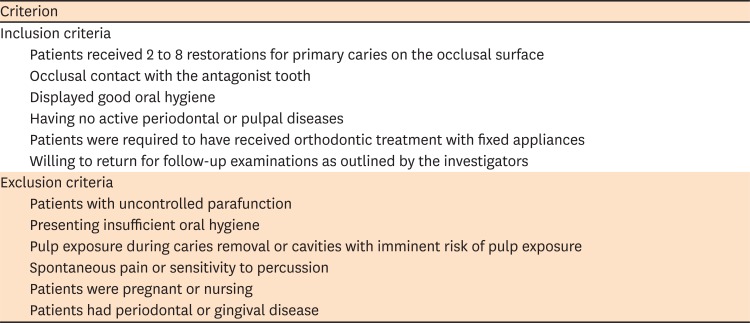
The study protocol was approved by the local ethics committee (Ethical Committee of Istanbul University; Reference number: 2008/696). Details of the materials used in the study (etchant, adhesive, and composites) are shown in Table 1. The restorations were placed between April 2008 and December 2009 at the Department of Restorative Dentistry, Istanbul University Faculty of Dentistry. A total of 28 patients (8 males and 20 females), who were going to commence orthodontic treatment and aged between 11 and 28 years (mean age: 16.8 years) were included in the study. All persons gave their informed consent prior to their inclusion in the study. A total of 118 occlusal caries restorations completed prior to orthodontic treatment were evaluated (Figure 1). Each patient received between 2 to 8 occlusal restorations. Patient inclusion and exclusion criteria are presented in Table 2 [7910]. All teeth had opposing and adjacent tooth contacts. Patients were required to receive treatment for all existing tooth caries on the occlusal surfaces of posterior teeth before beginning orthodontic treatment. Therefore, the interaction of the 2 disciplines was managed in the diagnosis and clinical treatment of these patients.
Table 1
The brand names, chemical compositions, application procedures, and manufacturers of the materials used in the study
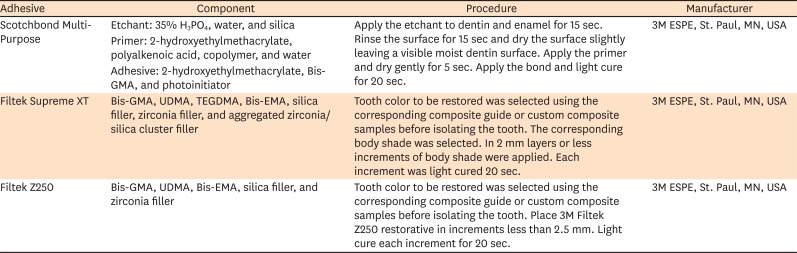
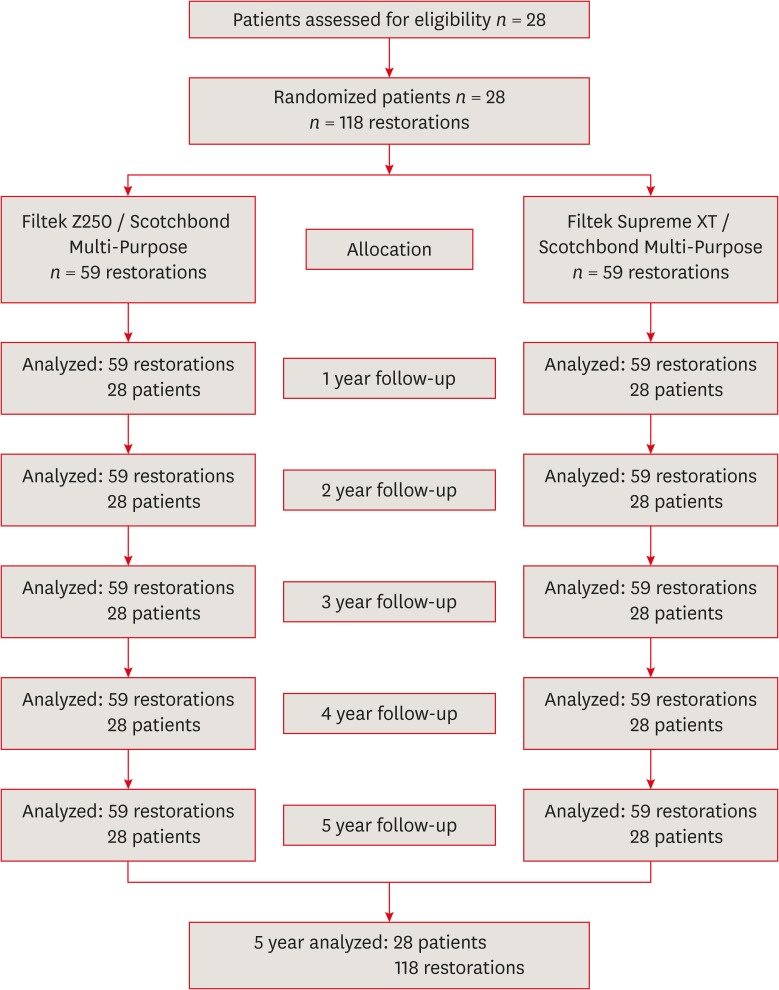
Table 2
Inclusion and exclusion criteria
Treatment protocol
According to the faculty's patient treatment protocol, the patients were first examined in the Department of Oral Diagnosis and Radiology, Istanbul University. After periapical and/or panoramic radiographs were taken, patients were referred to related departments. First, the teeth were cleaned using pumice-water slurry and a rubber cup to remove the pellicle and residual plaque. Lesions were diagnosed macroscopically under a dental operating light using plain dental mirrors, air syringes, and World Health Organization (WHO) periodontal probes to check for surface discontinuity. The lesions were identified as being cavitated, if they had reached the dentin (International Caries Detection and Assessment System [ICDAS] codes 3–5), but the lateral spread was limited to the dentin.
For the patients who received 2 occlusal restorations, one was performed with a nanofill resin composite (Filtek Supreme XT, 3M ESPE, St. Paul, MN, USA), while the other was performed with a microhybrid composite (Filtek Z250, 3M ESPE). The microhybrid and nanofill resin composites were applied in combination with a 3-step etch-and-rinse adhesive (Scotchbond Multi-Purpose, 3M ESPE) (Table 1). The microhybrid composite and tooth number were randomly selected by flipping a coin. This approach was first used for the patients with 2 restorations and the same randomized approach was then used to select the nanofill and microhybrid resin composites, and tooth number, respectively, for the patients with more than 2 restorations. After randomization, the number of restorations with Filtek Supreme XT per patient was equal to the number of Filtek Z250 restorations.
Cavity preparation was performed only for removal of caries and the cavity margins were not beveled. From each occlusal carious lesion, unsupported enamel rods were removed with minimal invasion using a cylindrical diamond bur (Komet, Gebr. Brasseler, Lemgo, Germany) in a high-speed handpiece under water cooling until the carious dentin was exposed. All of the cavities were prepared using round and cylindrical tungsten carbide burs (Komet, Gebr. Brasseler) in a low-speed contra-angle handpiece (maximum speed of 1,500 rpm) under air/water spray. Caries removal was ended, when a hard cavity floor was felt upon gentle pressure with a blunt dental explorer [11]. Cavity margins were not in occlusal contact. The cavities were categorized by depth as shallow (49 cavities), medium (31 cavities), or deep (38 cavities). The depth of the prepared cavity was measured against the mesial and distal marginal ridges using a graduated periodontal probe. According to this, > 2.5 mm cavities were classified as deep cavities, while < 2.5 mm as medium cavities and the dentin that neighbors the enamel as shallow cavities [12]. The average facio-lingual width of the cavities was between 1/3 and 2/3 of the intercuspal width. In deep cavities, a small amount of calcium hydroxide (Dycal, DeTrey/Dentsply, Konstanz, Germany) was placed on the deep portion of the cavity and then cavity floor was lined using a resin-modified glass ionomer cement (Vitrebond, 3M ESPE). Cavities considered as medium or shallow depth did not require lining. Cavity treatment and material application was performed according to the manufacturer's instructions by the same experienced practitioner (ST) who was familiar with both materials.
The shade was chosen using the corresponding guide or custom samples before isolation. Cavities were isolated using cotton rolls and saliva ejectors [13]. Scotchbond Multi-Purpose was applied to etched enamel and dentin in accordance with manufacturer's instructions (Table 1). The adhesive was light cured for 20 seconds using a halogen light curing unit (VIP, Bisco Inc., Schaumburg, IL, USA).
Either a microhybrid composite (Filtek Z250) or a nanofill resin composite (Filtek Supreme XT) was then applied in layers (maximum 2 mm) using an oblique incremental placement technique. Each increment of both composites was cured for 20 seconds. Halogen light intensity was checked with a radiometer (Hilux Curing Light Meter, Dental Benlioglu Inc., Ankara, Turkey) prior to and after curing to ensure that the output was at least 600 mW/cm2. After checking the occlusion and articulation, removal of excess material, contouring, and finishing were performed using microfine finishing diamonds ranging from fine to superfine (8368.204.023, Komet, Gebr. Brasseler). The restorations were completed by polishing using Sof-Lex abrasive disks (3M ESPE). After that, the patients received orthodontic treatment with fixed orthodontic appliances.
Evaluations
Two experienced calibrated examiners from the Department of Restorative Dentistry of Istanbul University evaluated the restorations using a dental explorer and mirror, in accordance with the modified United States Public Health Service (USPHS) criteria (Tables 3 and 4) [13141516]. The evaluations were made 1 week after restorations placement (baseline) and after 1, 2, 3, 4, and 5 years. The examiners were not involved in the restoration phase and were fully blinded to the experimental protocol. The 2 examiners studied a set of reference photographs to illustrate each score for each criterion. They then clinically evaluated 20 occlusal restorations together at 2 day intervals. The restorations are not presented in the current study. When a minimum 85% intra- and inter-examiner agreement was achieved in the calibration phase, the evaluation phase was commenced [16]. At baseline and 1, 2, 3, 4, and 5-year recalls, color match, wear or loss of form, discoloration, caries formation, marginal adaptation, and surface texture were evaluated and scored as Alpha, which represented perfect clinical form; Bravo, acceptable; Charlie, unacceptable and the restoration had to be replaced; Delta, which represented restoration fracture, mobility of the restoration, or the restoration was missing and required immediate replacement. Scoring conflicts were resolved through consensus.
Table 3
Direct clinical evaluation criteria (modified USPHS criteria) using visual inspection
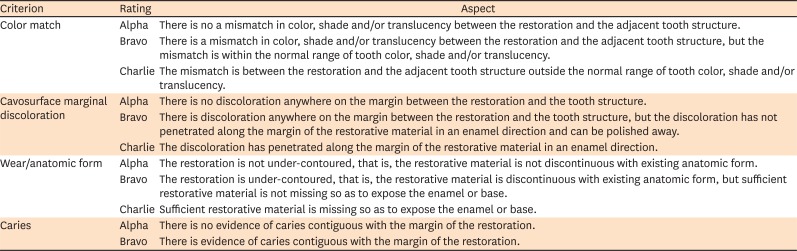
Table 4
Direct clinical evaluation criteria (modified Ryge criteria) using explorer

Statistical analysis
All analyses were performed using SPSS for Windows version 20.0 (SPSS, Chicago, IL, USA). Data obtained from each composite were statistically analyzed using the Friedman test to examine changes that occurred during the 5 years evaluation period. When a statistically significant difference was identified for any criterion assessed, the Dunn test was used for multiple comparisons between each recall time for each composite. The Mann-Whitney test was used to evaluate the differences between the 2 different composite materials. Kaplan-Meier survival analysis was used to determine the probability of the clinical survival of the 2 composites for a given time period. A p value less than 0.05 was considered statistically significant. Cohen's kappa was used to check for inter- and intra-examiner agreement.
RESULTS
The duration of orthodontic treatments ranged between 14 and 48 months (mean: 29.7 months). The distribution of occlusal restorations according to composite material types and teeth numbers are presented in Table 5. For the lower first molars, a few number of occlusal restorations were done. However, 69.5% of the restorations were done on the second molars. All patients attended the 1, 2, 3, 4, and 5-year recall visits, which resulted in a 100% recall rate for each evaluation period (Figure 1 and Table 6). Cohen's kappa (0.87) exhibited strong agreement between the examiners and no statistically significant difference was found between their evaluations (p > 0.05). The cumulative failure and retention (success) rates according to the Kaplan-Meier survival analysis are provided in Table 6. At each of the 5-year recalls, none of the restorations had failed, resulting in a 100% success rate for each evaluation period and a 100% cumulative success rate at the end of 5 years. Friedman test showed no significant differences between all of the evaluation periods of Filtek Z250 and Filtek Supreme XT restorations with respect to color match, marginal discoloration, wear or loss of anatomic form, caries, marginal adaptation, and surface texture.
Table 5
Distribution of occlusal restorations according to composite material type and tooth number

Table 6
Results of clinical evaluation of 2 different composite restorations using modified USPHS criteria
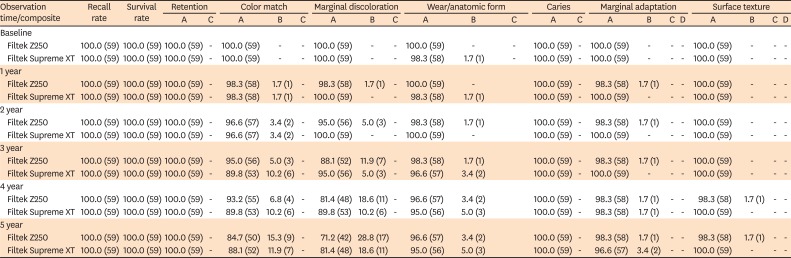
Five-year data of recall rate, survival rate, retention, color match, marginal discoloration, wear or loss of anatomic form, caries, marginal adaptation, and surface texture showed no statistically significant difference (p > 0.05).
USPHS, United States Public Health Service; A, Alpha; B, Bravo; C, Charlie; D, Delta.
Direct clinical evaluation results at baseline, and at the 1, 2, 3, 4, and 5-year recalls are shown in Table 6. None of the restorations were clinically unacceptable with regard to any evaluation criteria. Mann-Whitney test revealed there were no statistically significant differences in any of the clinical evaluation criteria between Filtek Z250 and Filtek Supreme XT restorations in each evaluation period. Regarding the color match, at the 5-year recall, 84.7% and 88.1% of the Filtek Z250 and Filtek Supreme XT restorations, respectively, were clinically ideal (Alpha). After 5 years, 28.8% of Filtek Z250 and 18.6% of Filtek Supreme XT restorations exhibited clinically acceptable marginal discoloration (Bravo). However, this discoloration was superficial, located on anywhere along the margin, did not penetrate towards the pulp along the margin of the restorative material, and could be polished away. With respect to wear and anatomic form, 96.6% of Filtek Z250 and 95% of Filtek Supreme XT restorations were clinically ideal (Alpha) after 5 years. Regarding the marginal adaptation rates, 98.3% of Filtek Z250 and 96.6% of Filtek Supreme XT restorations were clinically ideal (Alpha) at the 5-year recall. After 5 years, 98.3% of Filtek Z250 and 100% of Filtek Supreme XT restorations were clinically ideal (Alpha) with respect to surface texture.
DISCUSSION
In the present study, 2 types of resin composites were used in patients who were going to commence orthodontic treatment. Filtek Supreme XT nanofill resin composite contains nanometer sized particles (1–100 nm) throughout the resin matrix. Larger primary particles are not present. In microhybrid resin composite (Filtek Z250), the fine particles with an average particle size of 0.6 µm are blended with microfine silica [1718]. The 5-year survival rates of Filtek Z250 and Filtek Supreme XT restorations were 100%. No restorations failed, which meant an overall success rate of 100%. The change in performance between Filtek Z250 and Filtek Supreme XT restorations was only from clinically ideal (Alpha) to a clinically acceptable (Bravo) (not significant, Mann-Whitney test). In agreement with this finding, a nanofilled composite (Filtek Supreme XT) exhibited a success rate of 100% in occlusal and posterior approximal restorations after 5 years [19].
In contrast, a greater failure rate (6.4%) was reported for nanofill (Filtek Z350) and microhybrid (Filtek Z250) composites after 54 months in occlusal restorations [7]. However, in a 10-year retrospective study that investigated the longevity of posterior approximal restorations using 4 similar microhybrid resin composites, the overall survival rate was 97.9% and an improved performance was observed with Filtek Z250 restorations (99.1%) [20]. In contrast to this study, the present study evaluated 2 composites in occlusal cavities for 5 years. Cavity size played an important role on composite restoration survival. When compared with 1 surface restorations, the relative risk of failure has been reported to be approximately 2.3 times greater for 2 surface restorations and 3.3 times greater for multi-surface restorations [21]. It has also been documented that a reduction in cavity size protected the restoration from chewing forces [22]. Therefore, the size and type of cavity may have contributed to the high success rates in the present study. In accordance with this assumption, a review of 34 clinical studies performed over periods of at least 5 years found that 90% reported an annual failure rate between 1% and 3% for occlusal and posterior approximal composite restorations [23]. The variation in failure rates were dependent on several factors including tooth type and location, operator, and socioeconomic, demographic, and behavioral elements [23].
In the current study, 9 (15.3%) Filtek Z250 restorations and 7 (11.9%) Filtek Supreme XT restorations showed a change in color match after 5 years. This color change was clinically acceptable (Bravo) and did not necessitate restoration replacement. In contrast, another study reported no color change for a nanofill composite (Filtek Supreme XT) after 5 years in occlusal and posterior approximal restorations [19]. However, in support of the findings from the present study, 12.5% of microhybrid (Filtek Z250) and 6.5% of nanofill (Filtek Z350) composite restorations demonstrated acceptable color change after 54 months in occlusal cavities [7]. Staining would probably require a longer duration due to the transient nature of staining, and because saliva and other fluids dilute substances that stain and restorations are regularly cleaned through brushing. Therefore, color change may be due to pigment absorption or to dietary and oral hygiene habits [24].
In regards to marginal adaptation, 1.7% of Filtek Z250 and 3.4% of Filtek Supreme XT restorations exhibited Bravo scores, which showed visible evidence of a crevice along the margin into which the explorer could penetrate. Marginal discoloration also recorded Bravo scores in 28.8% of Filtek Z250 and 18.6% of Filtek Supreme XT restorations after 5 years. Most of Bravo ratings were shown in deep cavities. Deep cavities (39.4%) showed marginal discoloration and this was higher than medium (19.4%) and shallow (14.3%) cavities. Compared with the present study, a lower proportion of marginal discoloration and a reduced marginal deterioration rate (Bravo) have been reported after 54 months and after 5 years [719]. In contrast, a 10 year retrospective study of posterior composites demonstrated that marginal quality decreased with time because of physiologic and chemical reactions in the oral cavity, and degradation might indicate issues related to adhesive or resin composite [20].
After 5 years, only 3.4% of Filtek Z250 and 5% of Filtek Supreme XT restorations showed clinically acceptable (Bravo) wear or anatomic form. However, in a previous study, anatomic form deficiencies were recorded as Charlie in 6.5% of microhybrid (Filtek Z250) and nanofill (Filtek Z350) composites after 54 months [7]. However, this wear was more frequent and severe (Charlie) than in the present study. In contrast, another study reported that 2.2% and 2.7% of the posterior and hybrid composite restorations, respectively, were clinically acceptable (Bravo) anatomically after 4 years in occlusal and posterior approximal cavities [25]. It was indicated that anatomic form deficiencies in cases of 3 surface posterior restorations were greater than in 2 surface restorations, independent of the materials. This was accounted for by the greater resin composite surface, which wore after abrasive attack and led to material loss [20]. Therefore, in the present study, size and cavity type may have been contributing factors to the lower wear rates. In support of this, small-to-moderate sized posterior composite restorations were reported to have been used successfully for up to 20 years [26]. Seventy-six percent of the 85 restorations in their study were recalled after 17 years and were clinically acceptable. In addition, the effect of impact wear was stated to be limited owing to the moderate-to-narrow width of the restorations, which guaranteed that there was occlusal contact on tooth structure in almost every case [26].
In the present study, after 5 years only 1.7% of Filtek Z250 restorations was slightly pitted and exhibited rough surfaces (Bravo) that could be restored by polishing. In contrast, all Filtek Supreme XT restorations were clinically ideal (Alpha) with regards to surface texture. However, the incidence of clinically acceptable (Bravo) surface texture was previously reported greater for microhybrid and nanofill composites after 54 months and 5 years [719]. In agreement with our study, 97.4% of Filtek Z250 restorations showed no change and were clinically ideal in respect to surface roughness after 10 years [20]. In addition, 3 types of universal composites have been shown to exhibit a very high incidence of clinically ideal surface luster after 20 years [27]. Two previous studies also reported similar results after 17 and 22 years for posterior composites [2128]. Furthermore, in accordance with the findings of the present study, it was reported that fine-hybrid and nanohybrid composites exhibited ideal surface texture for all restorations (100%) in occlusal and posterior approximal cavities after 4 years [29]. Modern particulate resin composites have smooth surface characteristics after polishing [10]; therefore, reduced particle dimension and increased filler loading may have contributed to the higher incidences of clinically ideal surface texture in the present study. In addition, size and type of cavity may be factors that contribute to improvements in surface texture.
CONCLUSIONS
After 5 years, none of the microhybrid (Filtek Z250) and nanofill (Filtek Supreme XT) composites failed; the success rate was 100% for both composite materials. The composite restorations were clinically acceptable for all parameters at the end of the 5 years evaluation period. However, acceptable restoration rates (Bravo) were higher for marginal discoloration, followed by color match, compared with the other evaluation criteria. Modern composites such as the microhybrid and nanofill composites can result in high-quality restorations and produce positive long-term outcomes in occlusal cavities. In addition, orthodontic treatment did not affect clinical performance of 2 different composite restorations.
 XML Download
XML Download