

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Adequate knowledge of root canal system anatomy is indispensable to perform endodontic therapy.1 A major cause of root canal therapy failure is the inability to understand the internal anatomy of the tooth and subsequent incomplete endodontic treatment.2 A good pre-operative radiograph is essential for preventing missed anatomy but it does not always necessarily reveal the actual number of canals present in the root.3 Krasner and Rankow proposed specific laws of symmetry, law of color change, and laws of orifice location based on consistent and identifiable anatomic configurations of pulp chamber.4 These laws help to locate canal orifices on the pulp chamber floor in a systematic way. Visual and diagnostic aids also play an important role in detecting atypical root canal anatomy.5,6
Many investigations using different methodologies have been carried out to understand the internal anatomy of mandibular first molar. Although most prevalent root canal system configuration found are type IV and type I in mesial and distal roots respectively, it is common to find complex anatomy in mandibular first molar.7,8 Number of cases have been reported with more than 5 canals in mandibular first molar.9,10,11,12 Martinez-Berna and Badanelli reported 2 cases where 6 canals were present in mandibular first molar.9 Both the teeth had merging of the canals in distal root. Reeh reported presence of 7 canals in mandibular first molar with 4 canals in mesial root and 3 canals in distal root based on clinical and intra-oral periapical radiographic findings.10 Baziar et al. detected 6 canals in a mandibular first molar using CBCT, with 2 canals in mesial root and 4 canals in the distal root.12 However, following a Pubmed search, no cases reporting more than 7 canals could be found. This case report describes successful non surgical management of a mandibular first molar with 8 canals. Both the roots presented with type II configuration according to modified Vertucci classification.7
Case Report
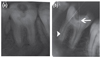
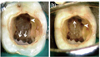
A 30 year-old female patient was referred by a local dentist to the Department of Conservative Dentistry and Endodontics with the chief complaint of continuous pain in lower left back tooth even after completion of the biomechanical preparation. On clinical examination, tenderness on vertical percussion was elicited on mandibular left first molar. Pre-operative radiograph (Figure 1a) and working length radiograph (Figure 1b) were provided by the previous dentist. The preoperative radiograph suffered from an artifact but working length radiograph revealed two important findings. Endodontic files were well short of apex in both roots, and roof of the pulp chamber was partially intact (Figure 1b). Based on the above findings, we could anticipate the reasons for the continuing symptoms. A diagnosis of irreversible pulpitis with apical periodontitis was formulated and completion of root canal treatment was planned. Inferior alveolar nerve block was administered using 2% Lignocaine with 1 : 80,000 epinephrine (Indoco Remedies Ltd., Mumbai, India) followed by isolation of the tooth using rubber dam. After removal of the temporary restoration, the remaining roof of the chamber was removed. Three canal orifices (mesiobuccal, mesiolingual and distolingual) were visible initially. Following the first law of symmetry reported by Krasner and Rankow, distobuccal canal was located in the first step (Figure 2a).4 In the second step, as the mesiobuccal and mesiolingual canals were widely separated, exploration using DG 16 explorer (Manipal Instruments, Manipal, Karnataka, India) was done at the floor wall junction as suggested by the first law of orifice location.4 Two additional canals were located between mesiobuccal and mesiolingual canals (Figure 2a). In the third step, exploration was carried out along the isthmus extending between and beyond the distolingual and distobuccal canals. Two additional canals were located, one buccal to the previously assumed distobuccal canal and the other one lingual to it (Figure 2b). Hence, a total of 8 canal orifices were located with 4 in each root. They were termed as mesiobuccal, linguo-mesiobuccal, bucco-mesiolingual and mesiolingual in mesial root, and distobuccal, linguodistobuccal, bucco-distolingual and distolingual in distal root according to proposed anatomically based nomenclature.13 Magnifying loupes (2.5X, STAC dental equipments Inc., Brampton, Canada) were used during the procedure. All the canals could be separately negotiated to a length of at least 17 mm from the orifice, beyond which merging of the canals was anticipated. Separate working length radiographs were taken for mesial (Figure 3a) and distal root (Figure 3b) as 8 files could not be accommodated together. This also helped in preventing overlapping of files' radiographic image. Radiographs clearly hinted towards existence of two separate foramina in each root. Working lengths for all mesial and distal canals were determined to be 19 and 19.5 mm respectively. Correlating the clinical and radiographic findings, the configuration of both roots was inferred as type 11 or 4-2.7 A cone beam computed tomography (CBCT) scan was required to confirm the anatomy but it was not feasible. Following working length determination, biomechanical preparation was completed using Protaper Ni-Ti rotary files (Dentsply Maillefer, Ballaigues, Switzerland). Irrigation was performed using 10 mL of 2.5% sodium hypochlorite solution and 10 mL of 17% ethylenediaminetetraacetic acid (EDTA) alternatively. Interappointment calcium hydroxide dressing was placed for two weeks. In the next appointment, following a final rinse with 4 mL of 2% chlorhexidine, all the canals were obturated with laterally compacted gutta-percha and AH plus sealer (Figures 4a and 4b). At 6 month follow-up visit, the tooth was found to be asymptomatic with normal radiographic periapical area (Figure 4c).
Discussion
In the present case, the canals could be located simply by following the guidelines of the pulp chamber floor anatomy and application of basic concepts.4 Additional canals in mandibular molars are generally hidden by a dentinal projection which is lighter in color as compared to the pulp chamber floor.3 This was clearly seen in the present case. Loupes were used during the procedure as microscope was not available. Although operative microscopes improve the probability of finding additional canals with decreased incidence of mishaps, it is proven that loupes also increase the possibility of detecting additional canals.5,14
In the mesial root of mandibular first molar, the presence of three canals is reported in many previous literatures.14,15,16 Most common configurations found in mesial root were type II and type IV.7 Four canals have also been reported in few case reports.10,17,18,19,20 In the distal root of mandibular first molar, presence of one canal has been the most common finding, but two canals have been found as high as 57.7% of molars in a study.5,21 Literature also exists confirming the presence of three and four canals in distal root.10,12,22,23,24 This is the first case reporting coexistence of 4 canals each in mesial and distal root of a mandibular first molar as no previous literature could be found following Pubmed search.
The uniqueness of the case is justified by the presence of 8 distinct orifices and type 11 or 4-2 configuration in both roots. The configuration of 4-2 has been mentioned as type VI in the Gulabivala et al.'s supplemental canal configurations and included in Vertucci modified classification as type 11.7,24 Such complicated anatomy is a consequence of secondary dentin deposition forming numerous partitions resulting in reticular form in which multiple vertical canals are present.25 An element of doubt was created by the radiographic image of files in distal root regarding existence of separate distolingual and bucco-distolingual canal. But, as all the orifices were separate and the canals could be individually instrumented to a minimum depth of 16 mm, it was legitimate to count all of them as separate canals. The above definitions have been used to identify a separate canal.26,27


 XML Download
XML Download