

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The histology of gastric adenocarcinoma varies. Within the group of well-differentiated adenocarcinomas, there is a rare variant characterized by fundic gland morphology [1234]. Gastric adenocarcinoma of the fundic gland type (GA-FG) was first described in 2010 [1]. The Japanese Classification of Gastric Carcinoma (JCGC) was recently revised and GA-FG was newly added as a special type [5]. The cells in these tumors show chief, parietal, or mucous neck cell differentiation and are typically mixed at various proportions [6]. GA-FG accounts for just 1.6% of all gastric adenocarcinomas [2]. Macroscopically, about 75% of GA-FG cases consist of a submucosal tumor (SMT)-like lesion, the remainder being flat or depressed [7]. These tumors are usually located in the upper third of the stomach and arise from the deep layer of the gastric mucosa [3]. According to most previous reports, GA-FG is of low-grade malignancy [248910]. It frequently invades the submucosa; however, invasion of the muscular or deeper layers is rare and lymph node (LN) involvement has not been reported.
Here we present a case of GA-FG that progressed to an aggressive cancer and metastasized to a LN. To the best of our knowledge, this is the first reported case of a GA-FG tumor with LN metastasis.
CASE REPORT
A 55-year-old man with a previous diagnosis of a gastric SMT visited our hospital 10 years after the identification of a gastric SMT that was detected in the posterior wall of the upper gastric body during a medical check-up (Fig. 1A). The tumor had not been followed up in the intervening 10 years because during that time he had developed myocardial infarction and chronic heart failure. However, 10 years after the original diagnosis, a follow-up gastroscopy in another hospital revealed an enlarged SMT with a rugged surface. An endoscopic fine-needle aspiration biopsy had been obtained, but the SMT could not be histologically identified. Therefore, he was referred to our hospital for further investigation.
Fig. 1
(A) Gastroscopy findings at the medical check-up during which the tumor was originally detected. (B) Gastroscopy findings 10 years later showing an enlarged submucosal tumor with evident morphological changes (arrows).
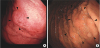
Gastroscopy at our hospital revealed a whitish elevated lesion in the posterior wall of the upper gastric body (Fig. 1B). No atrophic changes were evident. A histopathological examination of further biopsy specimens showed adenocarcinoma mimicking fundic glands and the tumor was diagnosed as a GA-FG. An endoscopic ultrasound study revealed a lowly echoic tumor and a thickened muscular layer consistent with a T2 invasion depth according to the JCGC 15th edition [5]. No enlarged LNs or other evidence of distant metastases were detected on a computed tomography scan.
The patient underwent a total gastrectomy with D2 lymphadenectomy. An intra-abdominal abscess developed postoperatively but resolved completely with percutaneous drainage.
Grossly, the tumor was a locally thickened lesion with indistinct borders measuring 4.7 cm in its largest dimension (Fig. 2). The gastric folds surrounding the lesion were slightly thickened.
Fig. 2
(A) The resected specimen consists of a locally thickened mass 4.7 cm in diameter located in the posterior wall of the upper gastric body. (B) The lesion borders are indistinct (arrows).

On low-power magnification, the submucosal layer was also thickened and the mucosa pushed up into the gastric cavity (Fig. 3A). Most of the tumor cells in the mucosal and shallow submucosal layers resembled mucous neck or chief cells with some intermingling eosinophilic cells resembling parietal cells (Fig. 3B and C). These cells formed densely aggregated glands with anastomoses. The tumor glands in the middle of the submucosal layer gradually transitioned into irregularly shaped tubular glands with surrounding desmoplastic reactions and lymph follicles (Fig. 3D). Some of these glands contained intraluminal necrotic debris (Fig. 3D). In the muscular and subserosal layers, the tumor cells formed predominantly isolated tubular glands or small clusters that diffusely and widely infiltrated these layers (Fig. 3E). Neural and venous invasion was detected within these layers (Fig. 3E and F) and lymphatic invasion was identified at the tumor's periphery. Among the 37 dissected LNs, a metastasis was identified at station No. 3a (Fig. 3G).
Fig. 3
Representative photomicrographs of gastric adenocarcinoma of the fundic gland type (GA-FG). (A) Low-power image of the tumor. In the top row, four lesions are indicated by squares and labeled B, C, D, and E; these correspond with the images in the bottom row (scale bar: 1 mm). (B) Mucosal and (C) submucosal tumor cells with round nuclei and predominantly basophilic cytoplasm. A few intermingled cells have eosinophilic cytoplasm. (D) Irregularly shaped glands with occasional anastomoses (left) that gradually transition into isolated dilated tubular glands (right). (E) Infiltrative component in the muscular layer. The inset shows neural invasion. (F) Cancer glands exhibiting venous invasion (arrowheads) confirmed by Elastica van Gieson staining. (G) Metastasis in a lymph node (arrowheads). The inset clearly demonstrates the cancer glands. Scale bars of the main images: 100 µm (scale bars of the insets: 50 µm for E, G and 20 µm for F).

Immunohistochemically, the mucous neck and chief cell-like cells in the mucosal and submucosal layers were widely positive for pepsin A; additionally, about half of these cells co-expressed MUC6 (Fig. 4C and E). The cells that resembled parietal cells were positive for H+/K+-ATPase but consistently negative for pepsin A and MUC6 (Fig. 4D). MUC5AC positivity was detected in only a few cancer cells (Fig. 4B). In contrast, the cancer cells in the muscular and subserosal layers were strongly and diffusely positive for MUC5AC and partially positive for MUC6 (Fig. 4H and I). Only a few cells in these layers were positive for pepsin A or H+/K+-ATPase (Fig. 4J and K). No aberrant expression of TP53 was identified. An attempt was made to identify the LN metastasis; however, no cancer cells were identified in the additional sections because the focus was very small.
Fig. 4
Immunohistochemically stained photomicrographs of cancer components in the mucosa (A-F) and subserosa (G-L). The tumor sections were stained for MUC5AC (B, H), MUC6 (C, I), H+/K+ ATP-ase (D, J), pepsin A (E, K), and Ki-67 (F, L) (scale bars: 50 µm).
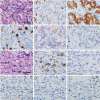
The Ki-67 labeling index of the tumor was approximately 1% within the tumor in the submucosa but as high as 5% within the tumor in the muscular and subserosal layers (Fig. 4F and L). These findings suggest that the GA-FG component in the mucosa and submucosa had transformed, forming an infiltrative tubular adenocarcinoma with foveolar epithelial differentiation that subsequently metastasized to a LN. Importantly, there was an obvious transition area between these two components in the submucosa, ruling out the possibility that the tumor was a collision cancer.
The pathological diagnosis was T3N1 according to JCGC criteria [5]. Nine weeks post-gastrectomy, the patient was started on adjuvant chemotherapy using S-1 alone. At the last follow-up 18 months later, there was no evidence of cancer relapse.
DISCUSSION
This case demonstrates that GA-FG has potential to progress to an aggressive cancer with LN metastasis. Although GA-FG frequently invades the submucosa, its progression is characteristically so slow that it is considered a low-grade malignancy [67891011]. There has been only 1 report of a GA-FG to date in which venous invasion was detected in a focus in the subserosa that seemed to be tubular adenocarcinoma without apparent fundic gland differentiation [12]. Given that GA-FG rarely invades the muscular layer and has not previously been reported to metastasize, treatment has typically consisted of endoscopic resection [6789]. However, the detection of a LN metastasis in our patient demonstrates that GA-FG can become an aggressive cancer with metastatic potential.
Because GA-FG is an uncommon neoplasm, its pathological diagnosis may be challenging. GA-FG typically includes tumor cells resembling chief, parietal, or mucous neck cells. These can be identified on hematoxylin and eosin-stained sections; however, immunohistochemistry is needed to confirm fundic gland differentiation. In our patient, the mucosal and submucosal cells of the tumor showed mucous neck or parietal cell differentiation confirmed by immunostaining for MUC6 and H+/K+-ATPase. We used anti-pepsin A antibody rather than pepsinogen-I, a precursor of pepsin A, as a marker of chief cells. Positive staining for pepsin A indicated chief cell differentiation. However, the cancer cells infiltrating the muscular and subserosal layers did not fulfill the diagnostic criteria for GA-FG because they lacked fundic gland differentiation. Rather, they were strongly positive for MUC5AC indicative of foveolar differentiation, which is frequently observed in conventional gastric-type adenocarcinoma [13]. Ueyama et al. [1] also reported foveolar differentiation within a GA-FG and suggested a shift in cell differentiation from the fundic gland type to the foveolar type during tumor progression. The present case is particularly informative in that it convincingly shows transformation of a GA-FG component into an infiltrative gastric-type adenocarcinoma with foveolar differentiation and LN metastasis. GA-FG with foveolar differentiation was previously reported as gastric adenocarcinoma of fundic gland mucosa type (GA-FGM) [14]. In that report, Tanabe et al. [14] described a GA-FGM with foveolar differentiation on the mucosal surface, which is a subtype of GA-FG. However, in the present case, there was no atypia in the surface foveolar epithelium. Because the definition of GA-FGM has not been well established, we cannot definitely determine whether the present case fulfills the diagnostic criteria for GA-FGM. Further investigations are needed to elucidate the differences between GA-FGM and GA-FG with foveolar differentiation and infiltrative transformation. Despite its resemblance to conventional gastric-type adenocarcinoma, the careful histologic examination of a gastric tumor is necessary to determine its true origin and determine whether it has progressed from GA-FG.
Although GA-FG has distinct phenotypic characteristics, no specific treatment strategy has been established. As with conventional gastric cancers, most patients with GA-FG are considered at minimal risk of developing metastases and have been treated by endoscopic submucosal dissection, the remainder undergoing surgical resection and LN dissection [148910]. In our clinical practice, the treatment strategy is chosen according to JCGC criteria [5] and the Gastric Cancer Treatment Guideline (GCTG) [15] but also considers the characteristic slow growth of GA-FG. Chiba et al. [16] prospectively followed 10 patients with GA-FG. No morphological changes occurred in any of these 10 patients during 16 months of endoscopic follow-up. In one study of 27 patients with GA-FG, the mean lesion size was 12.2 mm [17]. In our patient, the tumor had enlarged and become elevated during the 10-year interval without follow-up. The morphological changes presented here have not been reported previously and may be indicators of aggressive tumor transformation and the risk of LN metastasis. Therefore, even though most GA-FG tumors grow slowly, careful follow-up alone cannot be recommended. Rather, until GA-FG is better understood, local resection or gastrectomy with LN dissection should be performed at the time of diagnosis in accordance with the recommendation of the GCTG for common types of gastric cancer.
In conclusion, this case demonstrates the possible natural history of GA-FG, specifically its potential for transformation into an aggressive cancer with LN metastasis. Thus, GA-FG should not be managed by watchful waiting; rather, local treatment should be considered. Furthermore, according to the tumor's size, surface features, and estimated depth, gastrectomy with LN dissection similar to that performed for common types of gastric cancer should be considered. Further investigations are required to establish an adequate therapeutic strategy for GA-FG.
 XML Download
XML Download