

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Surgical resection is the only curative treatment for gastric cancer. Prognosis is generally poor; however, the number of patients experiencing long-term survival after gastrectomy for gastric cancer has been increasing owing to earlier diagnosis, improved surgical techniques, and advanced chemotherapeutic agents [12]. Nevertheless, while patients might be disease-free owing to surgery, most patients who undergo gastrectomy can suffer from various symptoms, including early satiety, loss of appetite, heartburn, dysphagia, nausea, and vomiting. Thus, it is crucial to pay greater attention to postoperative quality of life (QoL) in patients with gastric cancer [345].
Of the various tools used to assess QoL in patients with gastric cancer, the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire-Core 30 (QLQ-C30) and its gastric cancer-specific module (QLQ-STO22) have been used most frequently in previous studies [67]. These questionnaires have been translated into Korean, and their validity has been demonstrated [8].
Several studies that have used the EORTC QLQ-C30 and the QLQ-STO22 have reported long-term QoL following gastrectomy in patients with gastric cancer [391011]. However, most of these previous studies compared the overall scores, ranging from 0 to 100, according to the scoring manual provided by the EORTC. Assessing the frequency of each response is as integral to improving postoperative care, as is recognizing the changes in QoL over time. Therefore, we conducted the present study, with the aim of improving the QoL of patients undergoing distal gastrectomy, by investigating the proportion of questionnaire responses and comparing changes in QoL in long-term survivors following distal gastrectomy for gastric cancer.
MATERIALS AND METHODS
Participants
We enrolled patients with gastric cancer who underwent distal gastrectomy between January 2008 and June 2010 at Kyungpook National University Hospital (KNUH), in our study. We excluded patients with comorbidities such as cerebrovascular disease, cardiovascular disease, diabetes mellitus, chronic respiratory disease, or chronic hepatic disease, as well as those who underwent other operations. The 202 patients who completed the entire series of QoL assessments over 5 years were included in the final analysis. Table 1 shows the patients' demographic characteristics.
Table 1
Patient characteristics
QoL assessment
The Korean versions of the EORTC QLQ-C30 and QLQ-STO22 were used to assess patient QoL after distal gastrectomy. Patients were asked to complete the QLQ-C30 and QLQ-STO22 questionnaires preoperatively, and then over the 5 years after surgery. Questionnaires were completed by the patients themselves when they visited the outpatient department. If the questionnaires were returned with missing individual items, the patients were asked to complete those items. The functional and symptom scale items on the QLQ-C30 and QLQ-STO22 are rated from 1 to 4. The value of 1 represents “not at all”; 2 “a little”; 3 “quite a bit”; and 4 “very much.” All items except for global health status/QoL were classified into 3 subgroups: group I (good) for “not at all”; group II (fair) for “a little”; and group III (poor) for “quite a bit” or “very much.” Global health status/QoL was rated from 1 to 7. Patients reporting scores of 6 and 7 were included in group I (good); those reporting scores of 3, 4, and 5, in group II (fair); and those reporting score of 1 and 2, in group III (poor).
Statistical analysis
All patient characteristics are presented as a number (%), or mean±standard deviation. Global health status/QoL and all other scales were estimated as the mean proportion (%) of the number of patients responding in each component scale. All single items were estimated as the proportion (%) of the number of patients responding to each item measure. All analyses were conducted using SPSS software (version 22; SPSS Inc., Chicago, IL, USA).
RESULTS
Table 2 shows the proportions of patients in groups I, II, and III, for each of the EORTC QLQ-C30 and QLQ-STO22 functional and symptom scales/items at 5 years after surgery. Group I showed a tendency toward increasing global health status/QoL during the 5 years after surgery. The proportion of patients in group III for global health status/QoL was highest at 1 year after surgery (6.9%) and showed a tendency to decrease afterward (Fig. 1). Fig. 2 shows the changes in proportions of patients in group III for the functional EORTC QLQ-C30 scales. The proportion of patients in group III for the functional scales tended to decrease during the 5 years after surgery. The proportion of patients in group III for the physical functioning scales continuously decreased after surgery, and was similar to the preoperative proportion at 4 years after surgery (4.6%). The proportion of patients in group III for role functioning was maintained in the range of 3.8% to 4.5% during the 5 years after surgery. The proportion of patients in group III for emotional functioning was highest before surgery and steadily decreased to 3.5% after surgery. The proportion of patients in group III for cognitive functioning was highest at 3 years after surgery (7.1%) and decreased to 5.5% at 5 years after surgery. For social functioning, the proportion of patients in group III was lowest at 3 years after surgery and continuously increased to 5% at 5 years after surgery.
Table 2
Proportion of patients in each group on EORTC QLQ-C30 and EORTC QLQ-STO22 at 5 years after surgery
Fig. 1
Proportion of patients in each group for global health status/QoL scale of EORTC QLQ-C30 at each time point.
QoL = quality of life; EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30.
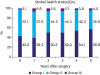
Fig. 2
Proportion of patients in group III for functional scales of EORTC QLQ-C30 at each time point. (A) physical functioning; (B) role functioning; (C) emotional functioning; (D) cognitive functioning; and (E) social functioning.
EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30.

Fig. 3 shows the changes in proportions of patients in group III for the EORTC QLQ-C30 symptom scales/items. The proportion of patients in group III for most symptom scales and items tended to increase 1 year after surgery compared to preoperative levels, and steadily decrease afterward. The proportion of patients in group III with fatigue was highest 1 year after surgery (14.6%) and decreased to 8.9% at 5 years after surgery. Proportions of patients in group III for insomnia and diarrhea items increased 1 year after surgery and gradually decreased during the 4 years after surgery (6.1% and 8.5%, respectively). At 5 years post-gastrectomy, the proportions of patients in group III with insomnia and diarrhea increased to 9% and 11.5%, respectively, which were higher than the preoperative levels.
Fig. 3
Proportion of patients in group III for symptom scales/items of EORTC QLQ-C30 at each time point. (A) fatigue; (B) nausea and vomiting; (C) pain; (D) dyspnea; (E) insomnia; (F) appetite loss; (G) constipation; (H) diarrhea; and (I) financial difficulties.
EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30.

Fig. 4 shows the changes in proportions of patients in group III for the QLQ-STO22 scales/items. The proportions of patients in group III with dysphagia, pain, reflux symptoms, and eating restriction scales were all less than 5% at 5 years after surgery. The proportion of patients in group III on the anxiety scale was highest 1 year after surgery and gradually decreased to 12.8% at 5 years after surgery. The proportions of patients in group III with dry mouth and taste at 5 years after surgery were similar to preoperative levels (10.5% and 2.0%, respectively). The proportions of patients in group III with body image problems and hair loss at 5 years after surgery were 9.9% and 12.6%, respectively.
Fig. 4
Proportion of patients in group III for scales of EORTC QLQ-STO22 at each time point. (A) dysphagia; (B) pain; (C) reflux symptoms; (D) eating restrictions; (E) anxiety; (F) dry mouth; (G) taste; (H) body image; and (I) hair loss.
EORTC QLQ-STO22 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire for gastric cancer-specific module.

DISCUSSION
Postoperative QoL in patients receiving gastrectomy is dependent on the extent of the gastric resection, the reconstruction type, and the abdominal approach method [1213141516]. Because QoL is one of the overall flow indicators for managing patients following gastrectomy, it is important to understand long-term chronological QoL changes, in general, after gastrectomy.
The present study determined the ratio of patients who suffered from poor postoperative QoL and suggested the optimal time to provide medical management for each of the functional and symptom scale items on the questionnaires. Patients in group I (who answered “not at all”) may rarely need medical support. Group II patients responded “a little,” and individuals in this group may occasionally need medical support and education for improving QoL. However, patients in group III (who answered “quite a bit” or “very much”) require appropriate medical support; it is important to follow up with these patients periodically. The symptoms of patients in group III should be the focus of individual management. Because such individual management for long-term survivors after gastrectomy is more demanding, an understanding of the overall changes in QoL following gastrectomy, as well as of the proportion of patients who experience impaired QoL at each time point after gastrectomy, is essential.
Similar to the findings of previous studies, the proportions of patients reporting good or fair global health status/QoL decreased slightly during the first postoperative year and tended to increase afterward [5]. Less than 5% of patients suffered from impaired global health status/QoL at 4 years after surgery. Physical, role, cognitive, and social functioning showed similar patterns. On these scales, about 4% to 7% of the patients showed poor QoL across the period of 5 years postoperatively. On symptom scales, the proportion of patients reporting poor QoL scores for nausea and vomiting, pain, dyspnea, appetite loss, and constipation items was 5% or less after surgery.
Previous studies showed that the emotional functioning score was lowest before surgery and improved gradually in the postoperative period [417]. In addition, the anxiety score was highest at 1 year after surgery, and decreased to the preoperative level 5 years after gastrectomy [1819]. Patients' worsened body image did not return to preoperative levels during the 5 years after gastrectomy [20]. In our study, changes in the proportions of patients reporting poor QoL in relation to emotional functioning, anxiety scale, and body image items were similar to those of previous studies. Although the scores on the emotional functioning and anxiety scales demonstrated recovery, 5.2% and 12.8% of patients had impaired QoL as assessed by the emotional and anxiety scales, respectively, at 5 years after gastrectomy. Furthermore, 9.9% of patients had a poorer body image 5 years after the operation. Emotional functioning and anxiety seem to be related to the depression caused by the initial cancer diagnosis; patients experience a feeling of relief from the disease-related depression over time. However, long-term survivors following gastrectomy have psychological difficulties related to issues such as tumor recurrence or fear of developing new cancer; these concerns might lead to impaired QoL in emotional functioning and anxiety. Thus, individual psychological counseling or supportive therapy aimed at relief from the disease may improve patients' emotional functioning and anxiety. In addition, the restoration of self-esteem with the support of psychosocial education may improve patients' body image.
Fatigue has usually been considered an unavoidable accompaniment to cancer, and its treatment may persist for years after cancer eradication [21]. In patients with cancer, fatigue has a considerable impact on self-care abilities and QoL [222324]. It is associated with many physical illnesses and psychological disorders that may affect physical sensations (e.g., feeling unable to perform tasks, weakness, and an unusual feeling of tiredness), affective sensations (decreased motivation, low mood, and lack of energy), and cognitive sensations (lack of concentration, difficulty thinking clearly) [2526]. The proportion of patients with poor fatigue scale scores in our study was highest 1 year after gastrectomy and remained at about 9% 5 years after surgery. As a result, patients who experience symptoms of fatigue following gastrectomy might have a deteriorated overall QoL in addition to their fatigue symptom scale scores. Patients with impaired fatigue scales should focus on their other QoL factors, and appropriate medical intervention such as non-drug treatments (e.g., exercise, rest, information, psychological interventions, and behavioral interventions) or pharmacological treatments (corticosteroids, progestational steroids, anabolic steroids, and psychostimulants) should be offered during the follow-up periods [21].
Cancer patients often feel free of disease when they have survived for 5 years after their surgeries. Although surviving 5 years after surgery is regarded as a turning point, impaired QoL has been observed to persist in survivors after gastrectomy [39]. In the present study, symptoms of impaired QoL such as fatigue, insomnia, diarrhea, anxiety, dry mouth, and body image bothered approximately 10% of patients during the 5 years after surgery. Management of these symptoms should be specifically targeted as part of long-term patient care following gastrectomy. Surgeons should be attentive to patients with these symptoms and provide appropriate intervention and individual management for each symptom. The main purpose of the QoL assessment for patients with cancer is to make the patient's discomfort known to the surgeon and to guide timely supportive postoperative care. Surgeons should reassure patients that QoL will return to good or fair levels by 5 years after surgery, although some impaired QoL or QoL deterioration related to upper gastrointestinal symptoms might persist; these symptoms of impaired QoL should be managed individually in a timely manner.
A limitation of the present study is that we could not assess QoL before the diagnosis of gastric cancer. QoL prior to the diagnosis of gastric cancer is generally the most valid baseline measure of a patient's QoL. Although the preoperative QoL was not altered by surgery, it might represent a patient's QoL after the diagnosis of gastric cancer. A preoperative-based interpretation of postoperative change in QoL may not only exaggerate the persistence of a decreased QoL but also conceal ongoing QoL deterioration after surgery [20]. However, obtaining data regarding patient QoL before the diagnosis of gastric cancer is not feasible in clinical practice. Thus, we considered preoperative QoL as baseline data. In addition, we excluded patients with comorbidities because QoL might be affected by such conditions, and we wished to focus on changes in QoL resulting solely from gastrectomy.
Another limitation of our study was that we were unable to determine why patients experienced poorer QoL at 5 years after surgery compared to 4 years after surgery on several QoL scales/items. All functional scales except cognitive functioning and the symptom items of dyspnea, insomnia, diarrhea, financial difficulties, and dry mouth tended to have the lowest proportion of patients with poor QoL at 4 years after surgery. The proportion of patients with poor QoL then increased 5 years after surgery. We hypothesized that this phenomenon might be related to the flow of emotional functioning and anxiety scale. As follow-up visits at 5 years after surgery are regarded as the last visit for primary cancer, patients might experience greater anxiety and nervousness about their cancer being completely cured. Further, increasing age might affect the QoL of long-term survivors.
Most patients in the present study had good or fair QoL after distal gastrectomy for gastric cancer. However, management of symptoms such as fatigue, insomnia, diarrhea, anxiety, dry mouth, and body image should be specifically targeted as part of long-term postoperative care for approximately 10% of patients. Nutritional support may improve fatigue, diarrhea, dry mouth, and body image. Psychological support may improve insomnia and anxiety.
 XML Download
XML Download