

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The presence of lymph node metastasis is an important factor in determining the stage and prognosis of gastric cancer patients.12 Therefore, meticulous lymph node dissection is essential for staging gastric cancer patients.
The tumor node metastasis (TNM) system has been widely used as a method for staging gastric cancer patients. The 7th edition of the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) TNM classification was released in 2010.3 According to this system, the N stage was classified into four pathologic stages (N0, N1, N2, and N3) based on the number of metastatic lymph nodes. However, at least 15 lymph nodes need to be harvested in order to apply this staging system.34
The total number of retrieved lymph nodes is influenced by the extent of lymph node dissection.56 The Japanese Gastric Cancer Association guidelines recommend D2 lymphadenectomy.7 Unlike eastern surgeons, western surgeons prefer to not perform D2 lymphadenectomy because of the associated high morbidity and mortality. As a result, many western gastric cancer patients have fewer than 15 total lymph nodes retrieved.68 Therefore, it has been suggested that the numeric concept of the 7th edition of the AJCC/UICC classification is not suitable in western countries.910 For this reason, the proportion of metastatic lymph nodes to examined lymph nodes (lymph node ratio) has been proposed as an alternative prognostic factor by western surgeons.11121314151617 Some surgeons have suggested that the lymph node ratio could be an alternative method to the established AJCC/UICC N classification. One report suggested that this ratio-based N (rN) staging classification could provide a more accurate estimation of overall survival without regard to the extent of lymph node dissection.12
In addition, the present AJCC/UICC classification has a problem of stage migration that appears to depend on the extent of lymphadenectomy.1217181920 It is assumed that this stage migration is due to the number of harvested lymph nodes. However, it is still uncertain whether a larger number of examined lymph nodes contributes to stage migration.
Therefore, in our study, we assessed the significance of the rN stage for the overall survival of our patients. We also evaluated whether rN stage with the elements of the numerical concept can more accurately classify N staging in gastric cancer patients.
Materials and Methods
1. Patients
We retrospectively reviewed and prospectively collected data on 222 advanced gastric cancer patients who underwent curative gastrectomy with lymph node dissection between January 2006 and December 2015 at Hanyang University Guri Hospital. All patients underwent over D1+beta lymphadenectomy according to the Japanese gastric cancer treatment guidelines.7 Laparoscopic gastrectomy was used for older patients and those with a high American Society of Anesthesiologist (ASA) score with the patients' consent.
2. Clinical analysis
Clinical data obtained from medical records included patient age, sex, body mass index (kg/m2), ASA score, and other data. The operative characteristics and early surgical outcomes included operation method (laparoscopic vs. open surgery), extent of gastrectomy (total vs. subtotal gastrectomy), omentectomy (total vs. partial), combined resection of other organs, operation time, postoperative complications, postoperative mortality, adjuvant chemotherapy, and overall survival were collected. The ASA classification was determined by anesthesiologists a day before surgery. Postoperative complications were defined as any condition requiring conservative or surgical treatment.21 Thirty-day mortality was used to measure postoperative mortality and it was defined as death within 30 days of the surgery. The overall survival was defined as the time from the operation to the date of the patient's death. Pathologic results were analyzed for tumor size, number of retrieved lymph nodes, and the 7th AJCC staging system score (pathologic T [pT] and pathologic N [pN]).3
In this study, we categorized our patients into 4 groups according to the lymph node ratio (the number of metastatic lymph nodes divided by the total number of retrieved lymph nodes, the rN stage). Our stratification reflected the 7th edition of the AJCC Cancer Staging (rN0, 0%; rN1 13.3%, 2/15; and rN2 40.0%, 6/15). As a result, our cut points were stratified into 4 grades (rN0, 0%; rN1, ≤13.3%; rN2, ≤40.0%; and rN3: >40.0%).
3. Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics ver. 21 (IBM Co., Armonk, NY, USA). All values are expressed as means with standard deviation. Categorical variables were analyzed using the chi-square test and all continuous variables were analyzed with Student's t-test. Survival analysis was performed by Kaplan-Meier curves with log-rank tests for significance. A P-value<0.05 was considered statistically significant.
Results
1. Clinical characteristics
The clinical characteristics of the 222 patients are shown in Table 1. The median age was 64.0 years. Men (71.6%) outnumbered women in this study population. Eighty-three patients (37.4%) underwent total gastrectomy. D2 lymphadenectomy was performed in most patients (90.5%). Fifty-two patients (23.4%) underwent combined resection of another organ and 77 patients (34.7%) underwent laparoscopic gastrectomy. The mean operation time was 212.5 minutes. Postoperative complications occurred in 41 patients (18.5%). There was no postoperative mortality in these patients.
2. Pathological characteristics
Table 2 shows the pathological characteristics of the patients. More than half of the patients had pT4 stage (55.0%) based on the 7th edition of AJCC/UICC. Less than half of the patients had pN3 stage (42.8%). The median number of retrieved lymph nodes was 42.5 (7~115). The majority of this study population (all except for four patients, 1.8%) had over 16 total retrieved lymph nodes.
3. Discordant correlation between pathologic N and ratio-based N in pathologic T4 gastric cancer patients
Based on the analyses that are shown in Table 3, the lymph node ratio for metastatic lymph nodes showed a large difference between the pN2 and pN3 groups. When using the rN stage for pN2 and pN3 patients, a downgrading of stage was observed in more than half of the patients.
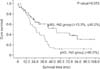
4. Comparison of pathologic T4N3 (Stage IIIc) gastric cancer patients according to the ratio-based N stage
Table 4 shows clinico-pathological characteristics between pT4rN2pN3 and pT4rN3pN3 gastric cancer patients. The 5-year overall survival (5-OS; 42.9% vs. 11.8%; P=0.013) was clearly different between the two groups. There were significant differences in the extent of gastrectomy (53.7% vs. 77.1%), tumor size (6.1 cm vs. 9.8 cm; P<0.001), N classification, and median number of metastatic lymph nodes (11 vs. 28; P<0.001). The two groups showed significant differences in overall survival (P=0.013; Fig. 1).
5. Overall survival of pathologic T4 gastric cancer patients according to the pathologic N and ratio-based N stage
As shown in Fig. 2, the survival curves based on rN classifications (5-OS; rN1 vs. rN2 vs. rN3, 70.8% vs. 48.0% vs. 12.2%; P<0.001) had a clearer distinction than those based on the pN classifications (pN1 vs. pN2 vs. pN 3, 82.5% vs. 64.8% vs. 27.2%; P=0.002).
Discussion
Accurate stage assessment is very important in prognostication and developing a treatment plan in gastric cancer patients. The 7th edition of the AJCC/UICC was released in 2010.3 Based on this system, the N stage is classified by the number of metastatic lymph nodes. However, more than 15 lymph nodes need to be harvested to apply this system, because of the possibility of down staging.34 Therefore, this numeric concept about the number of metastatic lymph nodes is difficult to use for gastric cancer patients with less than 15 retrieved lymph nodes.910
D2 lymphadenectomy is not often performed in western countries because of the associated high morbidity and mortality. Some western surgeons have suggested that extensive lymph node dissection does not improve overall survival.2223 As a result, there is a large difference in the total number of retrieved lymph nodes between Asian and western countries.6819 Therefore, many western surgeons raised concerns about the 7th edition of AJCC/UICC because of the down-staging of their patients.91017 They suggested that the lymph node ratio for metastatic lymph nodes could predict a more precise tumor stage for overall survival in their patients with fewer than 15 dissected lymph nodes.121415 In other words, many western studies have documented that the lymph node ratio is an independent prognostic factor that is not influenced by differences in the extent of lymph node dissection.
The total number of retrieved lymph nodes is affected by the extent of lymph node dissection.56 Although the effect of the total number of retrieved lymph nodes on overall survival is still a controversial subject, some study authors have suggested that dissecting a greater number of lymph nodes can improve overall survival of gastric cancer patients.2425 We believe that the lymph node ratio for metastatic lymph nodes could be a good alternative method to accurately evaluate staging, regardless of the total number of dissected lymph nodes.
However, in order to apply this ratio-based staging system in Asian countries, the cutoff levels need to be downgraded because of the large number of retrieved lymph nodes (total lymph nodes including negative lymph nodes). Our study found that almost all patients (98.2%) had more than 16 retrieved lymph nodes. Therefore, we applied the numeric concept of the 7th edition of AJCC/UICC system to our present study without using the previous cutoffs of western studies. We classified the rN stage into 4 categories (rN0 stage 0%; rN1 stage >0%, ≤13.3%; rN2 stage >13.3%, ≤40.0%; and rN3 stage >40.0%) by dividing pN (pN1 stage 2, pN2 6, and pN3 7) by the minimum number of lymph nodes, 15. As a result, we could achieve a lower cut-off value than that of the previous study.15
To explore the differences between pN and rN stages, gastric cancer patients with pT4 stage were reclassified according to their rN stages. Based on our results, over half of the pN2 and pN3 patients were downgraded from their original pN stages. We also confirmed that the simple numeric concept of the AJCC/UICC system does not accurately reflect the stage of pT4pN3 gastric cancer patients. There was a clear difference in the overall survival curve between the rN2 and rN3 groups in these patients (P=0.013). The rN3 group had poor overall survival, a higher rate of total gastrectomy, and a larger mean tumor size compared to patients in the rN2 group. In the comparison of the overall survival curves according to the pN and rN stages of pT4 gastric cancer patients, the rN stages also showed a clearer discrimination. Although our study did not show better survival outcomes in the lower stages of the pT4 gastric cancer patients, a previous study demonstrated that a good staging system must reflect decreased survival of patients with higher stages. That finding and the current study supports the idea that the pT4pN3 stage should be split into rN2 and rN3 classifications.26
After release of the 7th edition of the AJCC/UICC, many investigators have criticized the N classification system. Our results have confirmed that the present AJCC/UICC system has a serious issue with classification of accurate N staging. We also found that we had overestimated our patients' pN stages when using the 7th AJCC/UICC system. Although we confirmed that the lymph node ratio could be a good alternative method to decrease the possibility of stage migration, we still have some outstanding issues to resolve before applying the rN staging system in clinical practice. Although some western studies have documented that their cutoffs have significance for overall survival,15 it is very difficult to apply these cutoffs in Asian countries because of the differences in lymph node dissection. We believe that the difference in the number of retrieved lymph nodes should be considered in the next staging system. Therefore, an optimal Asian cutoff needs to be identified for use with different ethnic populations, one that is based on the extent of lymph node dissection.
This retrospective study has some limitations in the analysis of accurate rN stages. The system needs to reflect the better survival outcomes in the lower stage groups of pT4 gastric cancer patients. In addition, a study at multiple institutions with a larger patient cohort is needed to confirm the accuracy of the rN staging system in gastric cancer patients. In addition, we could not analyze patients at lower stages because of the small sample size. Therefore, we believe that a larger sample size is necessary to evaluate the impact of rN stages on overall survival of gastric cancer patients with less advanced stages (stage I, and II).
In conclusion, we have confirmed that the rN staging system can be a good alternative to the present AJCC/UICC staging system for pT4 gastric cancer patients. However, new cut-off values should be identified before applying this system to most Asian hospitals with a tendency to perform extensive lymph node dissection. Analysis of a larger group of patients is also needed to evaluate the impact of the rN staging system on less advanced stages.





 XML Download
XML Download