

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
According to the Korean National Cancer Incidence Database, gastric cancer was the second most prevalent cancer in Korea in 2010. The age-standardized incidence of gastric cancer per 100,000 people was 41.8 (men: 62.3, women: 24.9) in Korea in 2010. The detection of early stage gastric cancer has increased due to widespread cancer screening programs. However, many patients still die due to gastric cancer.1
The known factors that influence the survival of gastric cancer patients include distant metastasis, lymph node metastasis, depth of invasion, gross type, age, and type of resection.2 Besides these clinical factors, socioeconomic factors also affect the prognosis of cancer patients.3 In Korea, the entire population must enroll in the national health insurance (NHI) system, and those who are identified as having a lower socioeconomic status (SES) are supported by the medical aid (MA) system. Beneficiaries of the NHI system are entitled to insurance benefits and are required to contribute to the MA system financially, based on their wage or household income. In order to be eligible for MA, the poverty status of an individual must be annually assessed by the government.4
We aimed to determine the association of gastric cancer patients' survival after gastrectomy with their SES. Therefore, we analyzed the patients' medical insurance status as a parameter that reflects the patients' SES, and we retrospectively analyzed patient data.
Materials and Methods
A total of 333 patients who underwent gastrectomy for the treatment of gastric cancer between January 1999 and December 2010 at the Seoul Medical Center were reviewed. We excluded patients who had less than 15 lymph nodes (n=78) removed and patients who died within 30 days after gastrectomy (n=10); however, we included the cases of mortality among these patients when we calculated postoperative morbidity and mortality. Our hospital has adopted laparoscopic-assisted gastric surgery since June 2006. Nineteen patients (7.7%) underwent laparoscopic-assisted gastrectomy among a total of 247 patients during this study period. Among the 19 patients, 13 patients (7.1%) in the NHI group (183 cases) and 6 patients (9.3%) in the MA group (64 cases) underwent laparoscopic-assisted gastrectomy.
The data obtained for each patient included age, sex, body-mass index, levels of tumor markers (carcinoembryonic antigen [CEA] and carbohydrate antigen 19-9), tumor size, histologic type, and TNM gastric cancer stage classified according to staging criteria of the seventh edition of the American Joint Committee on Cancer. For the analysis of survival rates according to the SES, patients were classified into two groups based on their medical insurance status: the national health insurance group (NHIG) (n=183) and the medical aid covered group (MAG) (n=64).
Statistical analyses were performed using SPSS statistical software, version 12.0 for Windows (SPSS Inc., Chicago, IL, USA), with P-values <0.05 considered to be statistically significant. Continuous variables were expressed as medians with ranges. Categorical data were analyzed using the chi-square or Fisher exact test and continuous variables were compared using the Mann-Whitney U test. Survival rates were calculated using the Kaplan-Meier method and each group was compared using the log-rank test for univariate analysis and the Cox proportional-hazards model for multivariate analysis.
This study was conducted retrospectively after receiving permission from the local Institutional Review Board (No. 2013-048).
Results
The median patient age was 63.0 years (range: 31 to 87 years), and 70.4% of patients were male. The MAG patients comprised 25.9% of all patients in the study. Early gastric cancer (EGC) was noted in only 31.2% patients. The median value of the total length of hospital admission was 21 days (range: 10 to 236 days) (Table 1). According to the multivariate analysis of prognostic factors, the medical insurance status was found to be an independent prognostic factor for gastric cancer patients (P=0.009). Age (P=0.014), curability of operation (P<0.001), TNM stage (P=0.01), and Eastern Cooperative Oncology Group (ECOG) scale score (P=0.005) were also found to be independent prognostic factors in multivariate analysis (Table 2).
We compared various clinical characteristics between the NHIG and MAG. The ECOG performance scale score was lower in the MAG than in the NHIG (P<0.001). The EGC rate was not significantly lower in the MAG than in the NHIG (MAG: 25.0%, NHIG: 33.3%, P=0.279). The median preoperative serum hemoglobin (Hb) and albumin levels were lower in the MAG (MAG Hb: 11.45 g/dl, NHIG Hb: 12.5 g/dl, P=0.005; MAG albumin: 3.80 g/dl, NHIG albumin: 4.00 g/dl, P=0.027). The median postoperative hospitalization duration was longer in the MAG (MAG: 18 days, NHIG: 15 days, P=0.004). The rate of comorbidity was higher in the MAG (MAG: 51.6%, NHIG: 32.8%, P=0.012). The mean number of total retrieved lymph nodes during each operation was higher in the NHIG (NHIG: 33.18, MAG: 27.83, P=0.004). The median follow-up period was longer in the NHIG than in the MAG (NHIG: 74 months, MAG: 3.5 months, P=0.002) (Table 3).
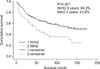
Operative mortality was higher in the MAG (MAG: 7 cases [9.9%], NHIG: 3 cases [1.6%]). The postoperative acute respiratory distress syndrome (ARDS) occurrence rate was higher in the MAG (MAG ARDS: 8.5%, NHIG ARDS: 1.6%, P=0.015) (Table 4). The overall 5-year survival rate was lower in the MAG (MAG: 43.9%, NHIG: 64.3%, P=0.001) (Fig. 1). Upon evaluating the TNM stage, patients in the NHIG showed longer survival than those in the MAG for every stage, but this difference was not significant for patients with stage III disease (Fig. 2).
Discussion
Known prognostic factors for gastrointestinal tract malignancies include TNM stage and performance status.1,2,5,6 In gastric cancer, the age, TNM stage, gross type, tumor location, tumor size, histologic classification according to the World Health Organization guidelines, operation method, postoperative complications, adjuvant chemotherapy, and lymphatic invasion also influence patient prognosis.7 In our study, the ECOG scale score, age, preoperative CEA level, and curability of the operation were found to be prognostic factors. This is similar to the results of previous studies, which reported that the poor performance status of patients who received adjuvant chemotherapy8,9 and increased levels of preoperative serum CEA10,11 are poor prognostic factors for gastric cancer patients.
The surgeon's experience is also another important factor influencing the patient's overall survival. In this study period, there were three surgeons who performed gastrectomy and the overall 5-year survival rate was not significantly different (staff A: 61.5%, staff B: 52%, staff C: 55.1%, P=0.191).
In addition to these clinicopathological factors, social and economic factors also affect the survival of gastric cancer patients. Several studies of the influence of SES on various malignancies have reported that mortality due to cancer was higher in patients with lower SES.3,12 In particular, there are many studies about the influence of socioeconomic disparity on the survival of breast cancer patients. According to these studies, the cause of higher mortality in lower SES patients was that the breast cancer was diagnosed in an advanced stage of the disease in lower SES patients13 and that there was a difference in the diagnostic procedure used or type of treatment received according to the SES.14 The existence of a disparity in outcomes according to the SES in other malignancies has also been reported. In prostate cancer, treatment with brachytherapy was affected by the patient's SES15 and the overall survival and sphincter preservation rates were lower in rectal cancer patients with lower SES.16
Regarding gastric cancer patients and their SES, Siemerink et al.17 reported that patients with a lower SES were diagnosed at an older age and had more distal tumors. In contrast, patients with a higher SES underwent resections and received chemotherapy more frequently. They also reported that the risk of dying was higher in patients with a lower SES, even after adjusting for confounding factors; as a result, SES was an independent prognostic factor for survival in patients with gastric cancer. Yim et al.3 reported that lower income is independently related to a shorter survival time in several cancers, including stomach cancer, in Korea.
The medical insurance status, which reflects the patient's SES, was found to be an independent prognostic factor in our study using multivariate analysis. The overall 5-year survival rate of the NHIG was 64.3%, but it was 43.9% in the MAG with P-value of 0.001. The hazard ratio for the overall survival rate of the MAG over the NHIG was 1.874. In order to understand this phenomenon, we analyzed differences in the distribution or level of various factors that might affect the prognosis of gastric cancer patients. As a result, the ECOG scale score, preoperative serum Hb and albumin levels, total and postoperative duration of hospitalization, rate of comorbidity, total number of retrieved lymph nodes per operation, follow-up period, rate of postoperative ARDS occurrence, total morbidity rate, and operative mortality rate were significantly different between the MAG and NHIG. Chemotherapy is also an important factor for predicting recurrence in advanced gastric cancer. We analyzed the difference in the rate of patients receiving postoperative adjuvant chemotherapy between the two groups, however, there was no significant difference (NHIG: 76.8% vs. MAG: 70.9%, P=0.513).
As mentioned above, the performance status is an independent prognostic factor. The ECOG scale score was lower in the MAG in our study can partially explain the survival disparity between the two groups.8,9
Lowrie and Lew18 reported that the mortality of patients with serum albumin levels between 3.5 to 4.0 g/dl increased two-fold compared to patients with serum albumin levels between 4.0 to 4.5 g/dl, and lower serum albumin levels were an independent risk factor for mortality. In our study, the median serum albumin and Hb levels were significantly lower in patients in the MAG than in those in the NHIG. This may reflect that the nutrition status of gastric cancer patients was poorer in the MAG than in the NHIG. Gastric cancer patients have a higher risk of malnutrition than do patients with other diseases.19 Furthermore, severe malnutrition can develop or be exacerbated by surgical treatment in gastric cancer patients.20 Not only can malnutrition limit the cancer treatments, but it can also act as a primary cause of death by increasing the rate of complications;21 a previous report indicated that 20% of all deaths of patients with malignancies were caused by deterioration of the patient's nutritional status rather than by the failure of the treatment for the malignancy.22 Therefore, nutritional support is important for gastric cancer patients who undergo gastrectomy. It is necessary to supply enteral feeding with immune-enhancing nutrients along with the appropriate use of appetite stimulants. Total parenteral nutrition should be reserved for patients with postoperative complications that delay enteral feeding for an extended period of time.23
The rate of comorbidity cases was higher in the MAG than in the NHIG. Comorbidities could contribute to the occurrence of postoperative complications, and they might also result in mortality due to causes unrelated to the cancer. Further, comorbidity could directly limit the patients' chemotherapy.
The operative mortality rate, postoperative pulmonary complication rate, and total postoperative complication rate were significantly higher in the MAG than in the NHIG (Table 3). The occurrence of postoperative complications in the MAG may also partly explain the poorer survival and the longer postoperative hospitalization duration in the MAG than in the NHIG.
The total number of retrieved lymph nodes was lower in the MAG than in the NHIG. This affected the survival of patients in the MAG in two ways; the first effect may be downstaging in patients in the MAG, as the number of lymph node metastases may have been undercounted. Therefore, it is possible that some patients in the MAG were classified as having a lower TNM stage than their actual stage, likely explaining the lower survival among patients with stage I and II disease in our study. The second effect might be the diminished therapeutic effect of the operation. The possibility of non-removal of lymph nodes that might contain metastatic malignant cells was increased in the MAG compared to the NHIG, and this might influence the overall survival of these patients.
Kwon et al.24 reported that higher income or higher education level correlated with higher participation rate in gastric cancer screening. According to the third Korean National Health and Nutritional Examination Survey conducted in 2005 by the Ministry of Health and Welfare, compliance with gastric cancer screening recommendations was approximately 33.2% for men and 29.6% for women. As expected, both men and women were significantly more likely to receive appropriate gastric cancer screening services with an increase in the household income.25 According to the report by Seo et al.,26 the rate of early gastric cancer diagnosis was significantly higher in the health screening group (79.1%) than in the non-health screening group (33.5%). In our study, the rate of patients who were diagnosed through the gastric cancer screening program was higher in the NHIG (37.6%) than in the MAG (14.7%) (P<0.001). The rate of EGC was 76.3% in the group of patients who were diagnosed with gastric cancer through screening programs and 21.4% in the group of patients who were diagnosed with gastric cancer through endoscopy after visiting a doctor due to gastrointestinal symptoms (P<0.001). As a result, in the current study, the rate of EGC was higher in the NHIG, which has higher rate of patients receiving gastric cancer diagnoses through screening programs, than in the MAG. Therefore, improving the quality of healthcare and access to screening programs is important for the population of lower SES. In the future, a more sophisticated investigation into the relation between the survival status and SES of gastric cancer patients is necessary.
The medical insurance status is an independent prognostic factor for gastric cancer survival. The overall survival of gastric cancer patients after gastrectomy was lower in the MAG than in the NHIG; this survival difference was observed for each TNM stage and the difference was particularly pronounced for stages I and II. In the MAG, postoperative morbidity and mortality were higher and poor prognostic factors were noticed more often. The SES may influence the survival of gastric cancer patients in Korea.





 XML Download
XML Download