

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Gastrointestinal stromal tumors (GISTs), which are the most common mesenchymal tumors arising within the gastrointestinal tract and a neoplasm differentiated through the malignant transformation of interstitial cells of Cajal (ICC). GISTs develop in decreasing order of frequency in the stomach, small intestine, large intestine, and esophagus; GISTs represent 0.1~0.3% of all gastrointestinal tumors.(1,2) The stomach is the most common site at which GISTs develop.(3)
GISTs are CD117 (c-kit)- or CD34-positive,(4) with positive rates of 94% and 60~70%, respectively.(5) Therefore, immunohistochemical staining allows a differential diagnosis between GISTs and existing submucosal tumors.
To predict the prognosis for these GISTs, pathologic factors, including the tumor size, mitotic count, c-kit mutation, tumor necrosis, cellular necrosis, interstitial necrosis, and lesion site are usually used, but such pathologic factors are not sufficient to make an objective prediction because GISTs exhibit various clinical features. A number of recent studies have evaluated the biological indices which are of use as prognostic factors in malignant tumors, such as gastric, lung, and breast cancers, for similar utility in the prognosis for GISTs, reporting the genetic mutation of c-kit and cell proliferation, including the Ki-67 proliferation index, proliferation cell nuclear antigen (PCNA), flow cytometry, and p53.(6-8)
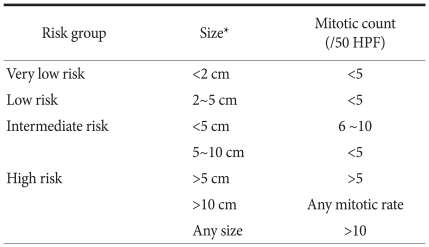
In predicting prognosis based on post-operative factors, Amin et al.(9) classified tumors into benign, borderline, and malignant based on tumor size and mitotic count, while the National Institutes of Health (NIH) consensus conference in 2001 divided the tumors into very low-, low-, intermediate-, and high-risk based on the risk of malignancy,(10) which is widely used for predicting post-operative malignant potential (Table 1). However, there is no method with which to predict the pre-operative prognosis for GISTs, with the exception of measuring tumor size using anatomic imaging techniques, such as computed tomography (CT), endoscopic ultrasonography (EUS), and magnetic resonance imaging (MRI).
Recently, the use of PET-CT as a non-invasive diagnostic tool in oncology for diagnosis and staging, as well as a technique to determine prognosis and the best course of treatment, has increased. PET-CT is expected to be useful as a non-invasive tool, especially for GISTs, because the pre-operative diagnosis, staging, and prediction of prognosis of GISTs is not easy.(11,12) Indeed, all GISTs have the potential for malignant transformation and there is no pre-operative diagnostic method that distinguishes GISTs from submucosal tumors.
The objective of the current study was to determine if PET-CT is clinically useful for predicting the pre-operative prognosis of GISTs by comparing the pre-operative maximum standardized uptake value (SUV) uptake (SUVmax) of the 18F-fluoro-2-deoxyglucose (FDG) PET-CT, which is a molecular imaging tool, with existing post-operative prognostic factors, such as the tumor size, mitotic count, and Ki-67 proliferation index, which is an immunologic index.
Materials and Methods
1. Patients
The study was conducted on 26 of 27 patients who were diagnosed with gastric submucosal tumors and underwent surgery after a pre-operative FDG PET-CT at the Catholic University of Daegue between Feburary 2007 and Feburary of 2009 (11 males and 16 females); 1 patient with a leiomyoma was excluded. The 2001 NIH risk classification (tumor size and mitotic count) and Ki-67 proliferation index were investigated regarding post-operative prognosis factors, and the correlation with the SUVmax of the FDG PET-CT as a pre-operative prognostic factor was retrospectively compared and analyzed. None of the patients had distant metastases. None of the patients had diabetes, and the blood glucose level in all patents were <100 mg/dl at the time of the PET scan. To evaluate malignant potential, we classified the NIH risk classification as "low-risk malignancy" (very low-risk and low-risk) and "high-risk malignancy" groups (intermediate-risk and high-risk). The study design was approved by the IRB of the Catholic University Medical Center of Daegu, and informed consent was obtained from all patients.
2. Diagnosis of gastric GIST
After the FDG PET-CT study, each patient underwent tumor resection. Eleven patients had laparoscopic wedge resections of the stomach, 13 patients had open wedge resections, and 2 patients had gastrectomies. Post-operatively, GIST was diagnosed by positive staining of c-kit, CD34, or both.
3. Ki-67 Immunohistochemisty
The surgical specimens were fixed with 10% neutral buffered formalin and embedded in paraffin blocks. Hematoxylin and eosin staining were performed. Immunohistochemical staining for c-kit and CD34 was performed by the standard avidin-biotin peroxidase complex method, and the Ki-67 proliferation index was determined. The Ki-67 index was defined as the percentage of nuclear-stained tumor cells per 1,000 tumor cells and evaluated by 1 pathologist to reduce bias.
4. PET-CT imaging
All patients fasted for at least 6 hours before the injection of tracer, then injected with 200 MBq of FDG. PET images were acquired 50 minutes after the administration of FDG. With the patient in the supine position on the scanner (GE Advance; GE Medical Systems, Milwaukee, WI, USA), a whole-body emission scan was obtained followed by a transmission scan for attenuation correction. A semi-quantitative analysis was simultaneously performed by calculating the SUV of FDG in the affected areas, as follows:

5. Statistical analysis
To test the association between pre-operative (the SUVmax of the PET-CT) and post-operative prognostic factors, we calculated Pearson's and Spearman's correlation coefficients. To determine the cut-off level of the MSU of the PET-CT, we retrospectively prepared a receiver-operating characteristic (ROC) curve based on the results. A P<0.05 was considered significant.
Results
1. Clinical characteristics of the patients
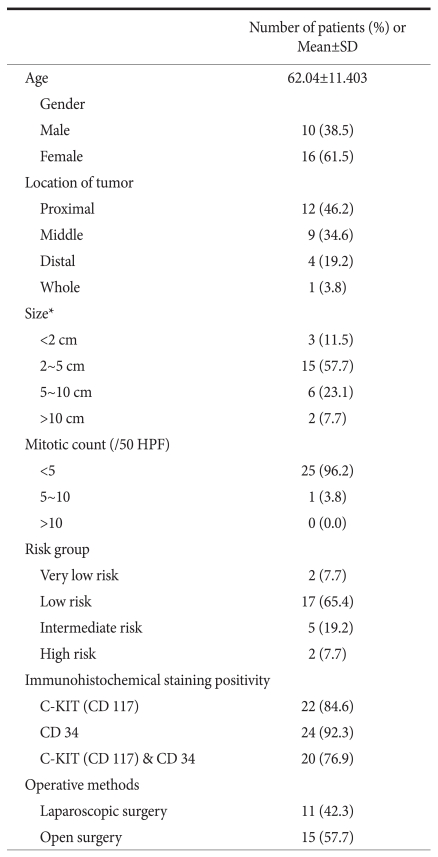
The clinico-pathologic characteristics of the 26 patients studied are summarized in Table 2. We studied 26 patients (10 males and 16 females) with a GIST of the stomach. The mean age was 62.04±11.4 years. All tumors stained positive for c-kit, CD 34, or both. FDG uptake was found demonstrated in all cases.
GISTs were primarily located in the proximal body (12 patients [46.2%]); the tumor size was 2~5 cm (15 patients [57.7%]). The majority of mitotic counts were 5/50 high-power fields (HPF), with none exceeding 10/50 HPF. The NIH risk classification was divided into very low- (2 patients [7.7%]), low- (17 patients [65.4%]), intermediate- (5 patients [19.2%]), and high-risk groups (2 patients [7.7%]).
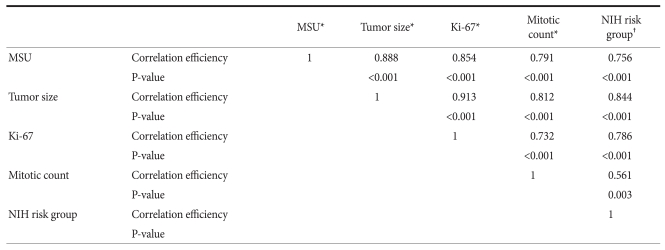
2. Relationship between maximum SUV uptake and clinicopathologic characteristics
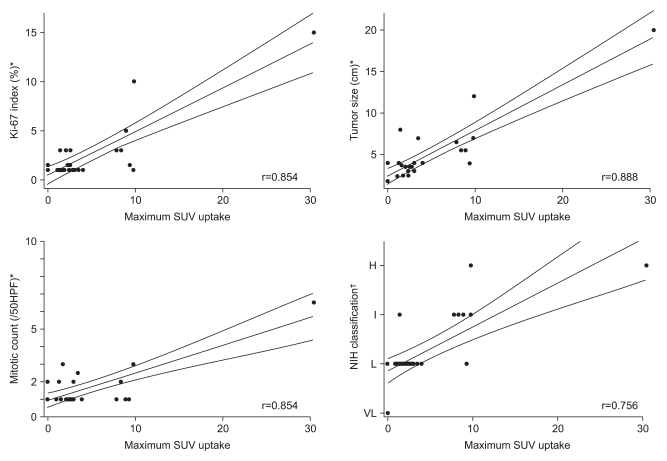
The relationships between the maximum SUV uptake and the clinicopathologic characteristics of gastric GISTs, including tumor size, Ki-67 index, mitotic count, and NIH risk group, are shown in Table 3. As a result of an analysis of the correlation between the maximum SUV and other prognostic factors, the correlation coefficient of the MSU with Ki-67, mitotic count, tumor size, and NIH risk classification was 0.854 (P=0.000), 0.888 (P=0.000), 0.791 (P=0.000), and 0.756 (P=0.000), respectively (Fig. 1).
3. Evaluation of the cut-off value
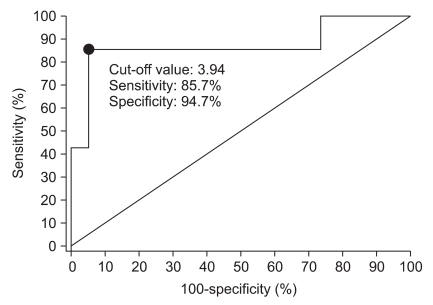
ROC curves were obtained by plotting a graph, in which the longitudinal axis showed sensitivity and the horizontal axis showed the false-positive rate. The nearest point to the left upper corner shows the most suitable cut-off point. To evaluate malignant potential, we classified the NIH risk classification as "low-risk malignancy" (very low-risk and low-risk) and "high-risk malignancy" groups (intermediate-risk and high-risk), and calculated the cut-off point. The cut-off value of the MSU was 3.94 between the "low-risk malignancy" and "high-risk malignancy" groups and the area under the ROC curve was 0.872. The sensitivity and specificity of the MSU for predicting the risk of malignancy were 85.7% and 94.7%, respectively (Fig. 2).
Discussion
Recently, many researchers have examined the post-operative indicators of malignant potential for GISTs, including the anatomic site, size, histomorphology, immunohistochemistry, and molecular genetics.(13) Size and an index of proliferation, either the Ki-67 index or mitotic activity, appear to be the most robust and useful prognostic factor post-operatively, even though recognizing absolute cut-offs are difficult to define. The outcome of the 2001 NIH workshop was the proposal of a classification of GISTs in terms of the relative risk of aggressive behavior, rather than simply benign or malignant.(10) Many parameters have been proposed, but the morphologic features that have gained greatest acceptance as predictive of outcome are mitotic rate and tumor size,(14-18) Although these indices correlate with a relative risk of malignant behavior, the fact remains that lesions that are very small (<2 cm) and lesions with very low mitotic rates (<5/50 HPF) occasionally metastasize. Furthermore, this phenomenon of unpredictability is not rare in patients with GISTs, and has led to the use of terms, such as uncertain malignant potential.(10) Therefore, every GIST is now considered to have uncertain malignant potential, and the malignant potential of a GIST is difficult to diagnose before surgery because the malignant potential is based on tumor diameter and mitotic index. It is relatively easy to calculate tumor diameter by anatomic imaging techniques, such as CT, EUS, and MRI, but not the mitotic index. This is a most important point regarding the need for pre-operative predictive factors of malignant potential.
PET with FDG is an imaging technology that has demonstrated clinical utility in the evaluation of gastrointestinal malignancies. A growing body of evidence supports the use of FDG PET as an accurate method to stage gastrointestinal malignancies. Tumors that demonstrate increased cellular metabolism are associated with increased glycolysis and increased glucose transporter proteins. After intravenous administration, FDG accumulates in tumors throughout the uptake phase, providing an integrated signal of high glycolytic tissue activity throughout the entire body. Thus, FDG PET could be a rapid, non-invasive method to demonstrate the glycolytic activity of a tumor and might be useful for assessing the malignant potential of a GIST. A markedly increased FDG uptake in GISTs has been documented in several studies and these studies indicated that FDG PET is useful for evaluating the effectiveness of imatinib mesylate, but not the malignant potential of the tumor.(19,20) In the current study we noted a significant correlation between FDG uptake and the mitotic rate, tumor diameter, and Ki-67 proliferation index (Fig. 1). The bioactivity of GIST had a correlation with FDG uptake because the mitosis reflected tumor cell proliferation, and the FDG uptake could evaluate the malignant potential of gastric GISTs if an FDG PET scan is obtained before surgery.
The cellular proliferative factors of GISTs include titrated thymidine, bromodeoxyuridine, Ki-67, and PCNA.(21) Ki-67 protein is present during all active phases of the cell cycle (G1, S, G2, and mitosis), but is absent from resting cells (G0). This antigen provides information regarding the proportion of active cells in the cell cycle and is an excellent marker for determining the so-called growth fraction of a given cell population.(22) The prognostic value of Ki-67 has been observed in cancers of the breast, prostate, cervix, and soft tissue.(23) Elevated Ki-67 expression has been shown to be associated with increased tumor aggressiveness and invasiveness. (24-26) In the current study, we noted a significant correlation between the Ki-67 index and SUV uptake (r=0.854, P<0.001), thus a high SUV uptake can be high cell proliferation, and higher aggressiveness and invasiveness; We therefore hypothesized that elevated SUV values occur in highly proliferative GISTs, and the results of the current study supported our hypothesis.
GISTs could be classified as low- (very low- or low-risk) and high-risk for malignancy (intermediate- or high-risk) groups. (10) We investigated the association between the MSU and risk categories based on morphologic features, including mitotic rate and tumor size by using ROC curves. The cut-off value of the MSU was 3.94 between very low- and low-, and intermediate- and high-risk groups based on the NIH risk classification (Fig. 2). With a similar aim, Yamada et al.(27) reported that the cut-off values of FDG SUV were 2.2, 4.2, and 6.5 for low-, intermediate-, and high-risk groups, respectively, which was very similar to our results (3.94 vs. 4.2). We believe that tumors with a MSU >3.94 have a high-grade of malignancy. Therefore, although additional studies are needed, FDG PET could to determine the management strategy for GISTs.
Many researchers have reported the malignancy or clinical behavior of GISTs.(5,18,28-30) At the European consensus meeting on the management of GISTs, it was suggested that all GISTs may need to be resected, but the controversy persists as to which is the best management strategy for relatively small lesions or those found incidentally during routine examinations because it is difficult to harvest a sufficient amount of tissue by endoscopic biopsy and predict malignant potentials of small GISTs, despite advances in molecular and immunohistochemical medicine. Recently, EUS-FNA was recommended as a safer technique that is essential for the pre-operative histologic diagnosis of gastrointestinal mesenchymal tumors.(27) At the European consensus meeting on the management of gastrointestinal mesenchymal tumors, no consensus was achieved among experts regarding the need for a pre-operative diagnosis by biopsies, obtained by endoscopic ultrasound or percutaneously because these tumors are very fragile, have the risk of tumor spillage, and may bleed easily.
FDG PET is a non-invasive modality. If a GIST shows heterogeneity, the metabolically active tissue can be distinguished from necrotic tissue by imaging the entire tumor in three dimensions. The maximum SUV of the tumor, rather than the average SUV, must be adopted for the analysis because the most metabolically-active regions of the tumor drive the overall behavior of the tumor and averaging active areas with areas of cystic change or necrosis (areas with a very low SUV) would result in falsely low overall values.(24) In the current study, therefore, one nuclear radiologist calculated the maximum SUV of the tumors in order to reduce bias.
In conclusion, The FDG PET scan is useful for assessing the bioactivity of gastric GISTs and less invasive than other techniques. Furthermore, it is easier to evaluate the malignant potential of gastric GISTs, and the sensitivity and specificity predicting risk of malignancy were 85.7% and 94.7%, respectively, if a FDG-PET scan is used before surgery. It is reasonable to expect a gastric GIST with a high FDG uptake to have malignant potential.
 XML Download
XML Download