

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Vitamin D deficiency is highly prevalent and has become an important health concern among Korean adolescents [1]. Vitamin D status has traditionally been considered an important factor in calcium-associated metabolism. In addition, recent attention has focused on the extra-skeletal effects of vitamin D [2] and increasing evidence has shown that low serum vitamin D levels were associated with obesity and metabolic syndrome [345].
Nonalcoholic fatty liver disease (NAFLD) is the most common hepatic disease in adolescents and its prevalence has risen substantially in recent decades [6]. Several different parallel processes participate in the development of NAFLD [7] and many potential risk factors for NAFLD, including obesity, insulin resistance, and metabolic syndrome, have been identified. Vitamin D deficiency has been investigated as a risk factor for the development of NAFLD and several studies have suggested that vitamin D levels were inversely associated with NAFLD in adults [891011]. However, few studies have investigated the relationship between vitamin D deficiency and NAFLD in an adolescent population [12].
This study aimed to elucidate the association between vitamin D deficiency and suspected NAFLD in adolescents using nationally-representative cross-sectional data after adjusting for obesity and metabolic syndrome.
MATERIALS AND METHODS
The Korean National Health and Nutrition Examination Survey (KNHANES), a South Korean national survey program conducted by the Korea Centers for Disease Control and Prevention, is an ongoing time-series cross-sectional and nationally-representative survey. The KNHANES obtains information using standardized health interviews, health examinations, and nutrition surveys. The data are collected annually from a complex, multistage, stratified, clustered probability sample, representative of the general Korean population [13]. The data on adolescents aged 12–18 years who participated in the KNHANES 2008–2014 (KNHANES IV–VI) were concatenated into one database.
The survey included 5,398 adolescents aged 12–18 years and 3,936 of the adolescents provided vitamin D blood samples. We excluded 44 adolescents with missing data on any relevant factors, as well as fourteen adolescents who were positive for hepatitis B surface antigen. As a result, 3,878 subjects were analyzed. Data regarding age, gender, body mass indexes (BMIs), systolic blood pressure (SBP), diastolic blood pressure (DBP), and waist circumferences were evaluated, as were data regarding glucose, cholesterol, high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), alanine transaminase (ALT), and vitamin D levels.
Suspected NAFLD was defined as a serum ALT level >30 U/L. Population studies have used serum ALT concentrations >30 U/L as surrogate markers for NAFLD in adolescents [1214]. The North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) guidelines for NAFLD suggest an ALT concentration >22 U/L for girls and >26 U/L for boys as a screening test for NAFLD [15]. Vitamin D levels were determined by measuring the level of serum 25-hydroxyvitamin D (25(OH)D), which reflects the vitamin D obtained by cutaneous synthesis and nutritional intake [2]. Serum 25(OH)D levels were measured by radioimmunoassay at the Neodyne Medical Research Laboratories and vitamin D deficiency was defined as a 25(OH)D concentration <20 ng/mL [2]. Anthropometric measurements were performed by medical staff according to a standardized protocol. Body weight, height, and waist circumference were measured to the nearest 0.1 kg, 0.1 cm, and 0.1 cm, respectively. Blood pressure was measured three times in the right arm and the final blood pressure value was obtained by averaging the second and third measurements. BMI was calculated using weight and height, and obesity was defined as a BMI ≥the 95th percentile for age and gender [16]. Data on adolescent BMI and waist circumference percentiles were obtained from the 2007 Korean National Growth Charts [17]. Metabolic syndrome was defined using the adolescent-specific criteria of the International Diabetes Federation and was diagnosed in adolescents with central obesity plus two or more of the other components or adolescents with four more of the other components [18].
This study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 1712-097-907). All participants provided informed consent.
Statistical analyses
Statistical analyses were carried out using SPSS software version 23.0 (IBM Corp., Armonk, NY, USA). We analyzed the risk factors for NAFLD using the Student's t-test (continuous variables) or χ2 tests (categorical variables). Continuous variables were reported as the mean±standard error and categorical variables were reported as counts and percentages. Univariate logistic regression analyses were conducted to identify the predictors of suspected NAFLD. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated using adjusted sample weights for the study population. Multivariate logistic regression analysis was used to analyze the association between vitamin D deficiency and suspected NAFLD after adjustment for all predictors that showed a significant association with suspected NAFLD in the univariate analysis. Sample weights were included in the analysis to account for the differential probabilities of selection, nonresponse, and noncoverage. Density plots for log-transformed ALT levels were generated using the R statistical package (R Foundation, Vienna, Austria). The p-values <0.05 were considered statistically significant.
RESULTS
The weighted and standardized prevalence of suspected NAFLD was 6.0 percent. Vitamin D deficiency was noted in 78.9% of the Korean adolescents. The prevalence of obesity and metabolic syndrome was 7.2% and 2.0%, respectively.
Table 1 shows the baseline participant characteristics according to the presence or absence of suspected NAFLD. Age, BMIs, waist circumferences, SBP levels, and DBP levels, as well as glucose, cholesterol, and TG levels, were higher in adolescents with suspected NAFLD than in adolescents without suspected NAFLD. HDL-C levels were negatively associated with suspected NAFLD. Adolescents with suspected NAFLD had significantly lower 25(OH)D levels than adolescents without suspected NAFLD (14.92±0.33 vs. 16.28±0.15 ng/mL, p<0.001). Male gender, obesity, metabolic syndrome, and vitamin D deficiency were positively associated with suspected NAFLD.
Table 1
Baseline characteristics of the participants according to the presence or absence of suspected nonalcoholic fatty liver disease
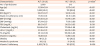
Categorical variables are shown as unweighted numbers of people and weighted percentages number (%), and continuous variables are shown as weighted means±standard errors in each group.
ALT: alanine transaminase, BMI: body mass index, SBP: systolic blood pressure, DBP: diastolic blood pressure, FBG: fasting blood glucose, HDL-C: high density lipoprotein cholesterol.
*Categorical variables were analyzed by Pearson χ2 tests, and continuous variables were analyzed by Student's t-test.
We generated a density plot to show the relationship between vitamin D deficiency and ALT levels. Because the serum ALT levels were log-normally distributed, we converted them into a log form, designated logeALT. The density plot was drawn by dividing the vitamin D-deficient and non-vitamin D-deficient adolescents into separate groups (Fig. 1). Vitamin D deficiency was more prevalent in adolescents with ALT levels above 30 U/L.
Fig. 1
The density plot of log-transformed ALT levels in adolescents according to the presence or absence of vitamin D deficiency. Vitamin D deficiency is more prevalent in adolescents with ALT levels above 30 U/L (p<0.01).
ALT: alanine transaminase.

We performed univariate and multivariate logistic regression analyses in which suspected NAFLD served as a dependent variable (Table 2). Univariate analysis showed that older age, male gender, obesity, metabolic syndrome, and vitamin D deficiency were significantly associated with suspected NAFLD and age- and gender-adjusted analysis showed that suspected NAFLD was significantly associated with obesity, metabolic syndrome, and vitamin D deficiency. Multivariate logistic regression analysis showed that increased age (OR, 1.17; 95% CI, 1.05–1.30) and male gender (OR, 5.63; 95% CI, 3.59–8.84) were independent determinants of the risk of suspected NAFLD. Obese adolescents were 8.29 times more likely to have suspected NAFLD than non-obese adolescents (95% CI, 5.24–13.12). Metabolic syndrome was independently associated with suspected NAFLD (OR, 3.86; 95% CI, 1.83–8.14). Adolescents with vitamin D deficiency were at higher risk for suspected NAFLD than adolescents without vitamin D deficiency (OR, 1.77; 95% CI, 1.07–2.95). Vitamin D deficiency in adolescents was also independently associated with suspected adolescent NAFLD when the NASPGHAN guideline for NAFLD was applied.
Table 2
Unadjusted, age- and gender-adjusted, and multivariate-adjusted ORs and CIs for suspected nonalcoholic fatty liver disease

DISCUSSION
The prevalence of vitamin D deficiency was 78.9% in the present study. In the United States (US) National Health and Nutrition Examination Survey 2001–2006, the prevalence of vitamin D deficiency in adolescent boys and girls was 28.1% and 34.3%, respectively [19]. In the KNHANES 2008–2009, vitamin D deficiency was noted in 75.3% of Korean adolescents, a finding similar to ours [20]. These results suggest that vitamin D deficiency was more prevalent in Korean adolescents than in US adolescents. The low vitamin D levels of Korean adolescents may be attributed to the enormous amounts of time that these individuals spend studying for their university entrance examinations and the limited amounts of time engaged in outdoor activities [21]. The prevalence of suspected NAFLD, defined as a serum ALT concentration >30 U/L, was 6.0% in Korean adolescents. The prevalence of suspected NAFLD was 8.4% in US adolescents 12–19 years of age [12]. A recent study showed that the prevalence of NAFLD in Korean adolescents 10–18 years of age did not change between 2001 and 2014 [22].
In this study, multivariate logistic regression analysis revealed that increased age, male gender, obesity, metabolic syndrome, and vitamin D deficiency were independently associated with suspected NAFLD. Our findings are supported by a prior study [14] showing that increased age and male gender were associated with suspected NAFLD in US adolescents. Among the independent correlates, obesity was the most serious risk factor for suspected NAFLD. The prevalence of obesity and metabolic syndrome is rapidly increasing in adults and adolescents [23]. Dysregulated adipokine production caused by excess adipose tissue triggers chronic low-grade inflammation and enhances insulin resistance [724], an integral feature of metabolic syndrome. NAFLD has been regarded as the liver manifestation of metabolic syndrome [25]. Our data revealed an adjusted OR of 3.86 for the association between metabolic syndrome and suspected NAFLD in adolescents. Previous studies have also demonstrated this strong association, with metabolic syndrome being more prevalent in Korean and US adolescents with suspected NAFLD than in Korean and US adolescents without suspected NAFLD [2627]. In addition, metabolic syndrome was positively associated with the severity of NAFLD in children [28].
Vitamin D levels were inversely associated with obesity, insulin resistance, and metabolic syndrome [34]. Therefore, obesity and metabolic syndrome might confound the association between vitamin D deficiency and NAFLD. In this study, we controlled for obesity and metabolic syndrome as confounding variables. We demonstrated for the first time that vitamin D deficiency was significantly associated with suspected NAFLD in adolescents after adjustment for obesity and metabolic syndrome.
Several studies have shown that serum vitamin D levels were related to NAFLD. Adult population-based studies have noted that low vitamin D levels were independently related to NAFLD [891011] and a study of Korean adults showed that vitamin D deficiency was significantly related to NAFLD in men but not in women [29]. However, serum vitamin D levels were not significantly associated with NAFLD in a Chinese adult population [30]. A meta-analysis including nine studies demonstrated that the risk of vitamin D deficiency was 26% higher in subjects with NAFLD than in control subjects [31]. Low vitamin D levels were independently associated with liver biopsy-proven NAFLD in adolescents [32]. In another study, low vitamin D levels were not found to be an independent predictor of suspected NAFLD in 1,630 adolescents after adjusting for obesity [12]. Our study had a relatively larger sample size than the US study and was adjusted for metabolic syndrome, in addition to obesity.
The mechanisms underlying the association between low vitamin D levels and NAFLD are largely unknown. Some studies have revealed that low vitamin D levels decreased insulin sensitivity and impaired beta cell function [33], suggesting that low vitamin D levels participate in the development of NAFLD by increasing insulin resistance. However, the finding that vitamin D deficiency was independently associated with suspected NAFLD after adjusting for metabolic syndrome, a phenotypic marker of insulin resistance, suggested that vitamin D was directly involved in the development of NAFLD. In rats exposed to a Westernized diet, low vitamin D levels led to the aggravation of hepatic steatosis and lobular inflammation. Low vitamin D levels also led to an increase in markers of the Toll-like receptor signaling pathway, suggesting that low vitamin D levels can lead to hepatic steatosis by activating Toll-like receptors and downstream inflammatory signaling molecules [34]. In rat models of diet-induced and obesity-related nonalcoholic steatohepatitis, nonalcoholic steatohepatitis progression, but not obesity progression, was attenuated by phototherapy, suggesting that vitamin D had anti-inflammatory activity, rather than anti-obesity activity [35].
In addition, a lack of outdoor activities in children with obesity can be another cause of vitamin D deficiency. For decades, the prevalence of obesity has been rapidly increasing, while physical activities, such as active transport or physical education in school, have decreased in children [3637] and many studies have shown that obesity was associated with lower levels of physical activity and more screen media exposure in school-aged children [3839]. In this regard, reducing screen time and increasing outdoor activities should be recommended for children with obesity and vitamin D deficiencies.
Our findings regarding the relationship between vitamin D deficiency and NAFLD suggest that taking vitamin D supplements represents a therapeutic option for patients with NAFLD. Hepatic steatosis severity was found to significantly improve after four weeks of vitamin D supplementation [40]. Additional studies are required to determine the therapeutic effects of vitamin D supplementation on NAFLD in adolescents.
The major strength of this study was that it is the first nationally-representative study outside the West to show an association between vitamin D deficiency and suspected NAFLD in adolescents. We conducted the analysis over a 7-year time period using composite stratified extraction and sample weights representative of the Korean adolescent population. This study was also the first to investigate the association between vitamin D deficiency and NAFLD in adolescents after adjusting for obesity and metabolic syndrome.
This study had some limitations. First, the diagnosis of NAFLD was not confirmed by liver biopsy. The gold standard for the diagnosis of NAFLD is a liver biopsy, however, the procedure was not feasible in this population study. Elevated ALT levels are widely accepted biomarkers for NAFLD in population-based studies [11121426]. The main purpose of this study was to reveal the association between vitamin D deficiency and suspected NAFLD, rather than to assess the prevalence of suspected NAFLD. Second, whether a causal relationship exists between vitamin D and NAFLD could not be determined from this observational, cross-sectional study.
In conclusion, increased age, male gender, obesity, and metabolic syndrome were found to be independent risk factors for suspected NAFLD in our nationally-representative sample of Korean adolescents. Vitamin D deficiency was associated with suspected NAFLD, independent of obesity and metabolic syndrome.
 XML Download
XML Download